Bowel Obstruction / Ileus
- Paralytic ileus
- Bowel obstruction
- Small bowel
- Large bowel
- When the bowels are prominent with air you have to distinguish it from small bowel obstruction, large bowel obstruction and paralytic ileus. You can make image based conclusion by paying attention to:
- Which bowel is prominent small or large
- Is it dilated or normal in size
- Is there air in the rectum or not
Obviously history and physical examination, bowel sounds are critical for the final diagnosis.
What are the sites of bowel obstruction?
What are the radiological findings of paralytic ileus?
- Distended bowel with multiple air-fluid levels
- Gas seen in the rectum
How is bowel obstruction different from paralytic ileus?
- There will be paucity of gas in bowel beyond the site of obstruction, unlike in paralytic ileus where gas can be seen in the rectum.
What are the common causes of paralytic ileus?
- Paralytic ileus occurs when there is inflammation in the peritoneum, most often following abdominal surgery, or other inflammations, like appendicitis, pancreatitis, etc.
- Normal postoperative ileus lasts 48 hours.
- The absence of bowel sounds, flatus, or bowel movements beyond the expected period indicates delayed resolution or bowel obstruction.
What are the common causes of small bowel obstruction?
- Post-op adhesions
- Gallstone ileus
- Intussusception
- Tumors
What are the common causes of large bowel obstruction?
- Cancer colon
- Fecal impaction
- Diverticulitis
What are the useful imaging procedures in the evaluation of bowel obstruction?
- Plain film serves as a screening procedure to detect bowel obstruction.
- Supine and erect films are often done to look for dilated loops of bowel and air fluid levels.
- However, comparing various studies of the efficacy of plain abdominal films in working up SBO show a wide range of sensitivity and specificity.
- Sensitivities ranged from 41 to 86% and specificities range from 25 to 88%.
- CT abdomen provides detailed information including the possible etiology for obstruction.
- CT with PO and IV contrast has a sensitivity and specificity of 100 and 83%. If the bowel is ischemic, then specificity decreases to 61%.
- Lower GI is rarely done nowadays.
What are the radiological findings of small bowel obstruction?
The characteristics of small bowel obstruction include:
- Multiple air-fluid levels
- Stacked
- Centrally located loops of intestine
- Dilated small bowel greater than 3 cms visible with valvulae conniventes.
- String of pearl sign caused by slow resorption of intraluminal air leaving small air bubbles trapped between valvulae conniventes
- Absence or paucity of colon gas: Collapsed colon
What are the radiological findings of large bowel obstruction?
- Obstructed colon usually appears as a peripherally located distended bowel with haustral markings.
- No air distal to site of obstruction.
- Sometimes the mass may be seen.
How do you distinguish small from large bowel?
- Small bowel is in the central abdomen.
- Large bowel is in the periphery of abdomen.
- Valvulae Conniventes crosses the entire width of small bowel.
- Haustra are seen partially across the width of large bowel.
- Bubbly appearance of feces indicates large bowel.
- Diverticula are present only in large bowel.
Image Atlas for Bowel Obstruction / Ileus

CT With GI Contrast
Normal Bowel
- Large bowel is identified by the sacculations called haustra scattered all along the colon.
- The colon has fat filled tags called appendices epiploicae on its surface.
- These haustra and epiploicae separate the large from the small intestine.
- Colon is filled with feces which has bubbly appearance
- The small bowel is located in the center of abdomen.
- Fairly narrow about 2.5 cm tube like structure winds compactly back and forth within the abdominal cavity.
- The small intestine is identified by valvulae circulares or circular folds on oral contrast study.

Plain film in a case with Small bowel obstruction
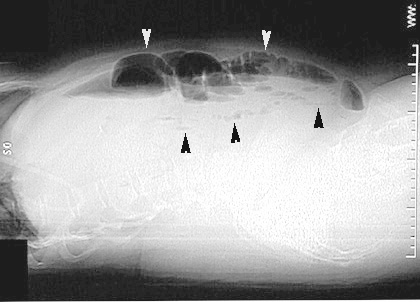
Post-Op Paralytic Ileus
- Multiple dilated small bowel loops are seen (white arrowheads).
- There is fecal material in the right and left colon
(arrows). - Air is seen in the rectum.
- The surgical staples indicate recent abdominal surgery. (black arrowheads).
Small bowel obstruction
Cross lateral view shows multiple dilated fluid filled loops of bowel with air fluid levels.

Small bowel obstruction
Absence or paucity of colon gas
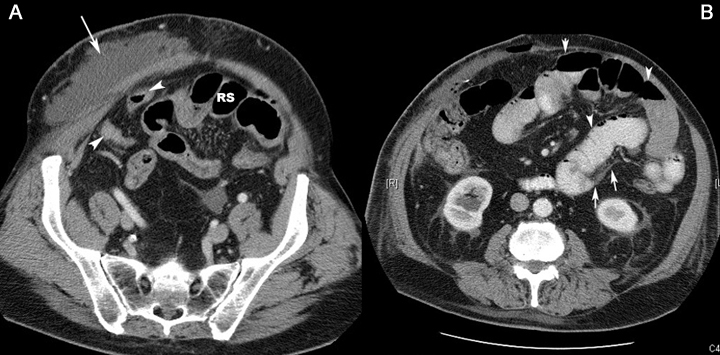
CT scan of another patient showing findings of small bowel obstruction:
- Post-op changes in abdominal wall
Arrowheads: Normal size of distal small bowel and rectosigmoid (RS) - Arrowheads: Dilated small bowel loops
Arrow: Area of obstruction
Small bowel obstruction
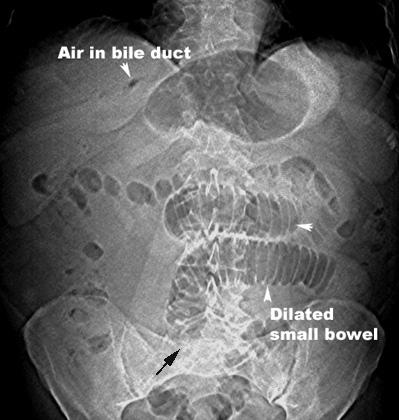
Gallstone Ileus
- Air in bile duct
- Dilated small bowel
- Gallstone is not seen in this film and may overlie the sacrum where the dilated bowel seems to end (black arrow)
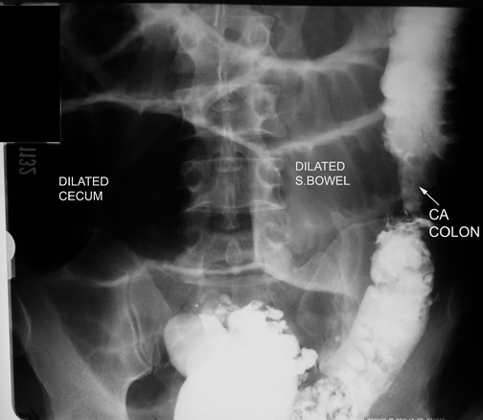
Lower GI in a patient with Large bowel Obstruction
- Dilated bowel loops proximal to the obstruction
- Arrow points to the etiology of obstruction