Figure 1
Epidural Abscess
Case 1:
60 year old patient with fever and paraparesis following placement of an epidural catheter placed to deliver pain medications for an uncontrollable back pain from pancreatic carcinoma.
Imaging findings: Figure 1
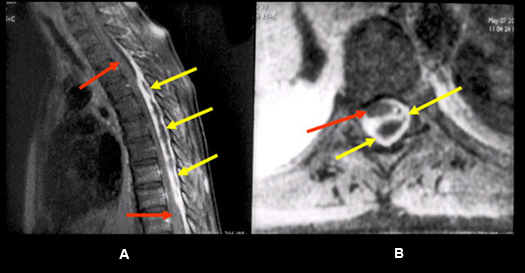
- Post-contrast sagittal T1wtd. MRI of thoracic spine
- Post-contrast axial T1wtd. MRI
- The capsule of the abscess (yellow arrows) enhances intensely with central low signal intensity produced by pus.
- Cord (red arrows) is displaced anteriorly by dorsally located epidural abscess (yellow arrows).
Diagnosis is based on clinical history and should not be confused with epidural tumors. Capsule of the abscess enhances while the central purulent portion doesn't, thus demonstrates ring enhancement. Epidural tumors usually demonstrate diffuse solid enhancement.
Imaging findings are consistent with an epidural abscess.

Figure 2
Osteomyelitis
Case 2:
30 year old patient with fever and upper back pain. History of intravenous drug use.
Imaging findings: Figure 2
- Sagittal T2 wtd. MRI
- Post-contrast sagittal T1wtd. MRI
- Pre-contrast axial T1wtd. MRI
- Post-contrast axial T1wtd. MRI
Imaging characteristics of osteomyelitis include abnormal low signal intensity involving adjacent vertebral bodies and the disc space as noted on T1wtd. image (yellow arrows in fig. C), hyperintense signal on T2 wtd. image (small yellow arrows point to the vertebral bodies and large arrow points to the disc space in fi.g A).
Post-contrast images demonstrate abnormal enhancement involving the adjacent vertebral bodies (small yellow arrows in figures B, D) and disc space (large yellow arrow in fig. B).
Prevertebral components of abscess is shown by white arrows in fig. D.