 |
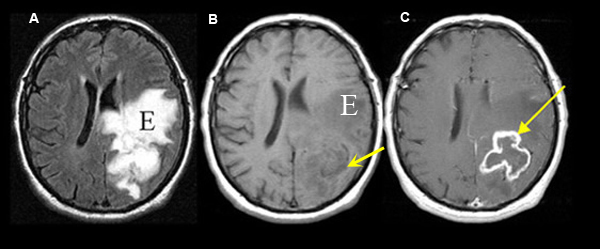
Figure 1 A: Axial flair MRI |
Glioblastoma
Case 1:
Imaging findings: Figure 1
- An irregular enhancing ring lesion (arrow in C) is seen involving the left parietal lobe in post-contrast axial T1 wtd. MRI, but poorly visible on pre-contrast T1 wtd. image (arrow in B).
- Tumor is associated with edema (E) and better noticed on FLAIR image (A), compared to T1 wtd. image (E in B)
Final impression:
Glioblastoma involving the left parietal lobe.
It's usually an irregular solitary mass, often with necrosis and surrounding edema. Presents as a mass lesion with symptoms dependent on its location (head aches, seizures, hemiparesis, sensory or visual deficit, behavioral change etc).
Differential diagnosis of enhancing ring lesions:
- Irregularly enhancing ring mass:
- Glioblastoma
- Circumscribed enhancing ring lesions:
- Metastasis
- Abscess
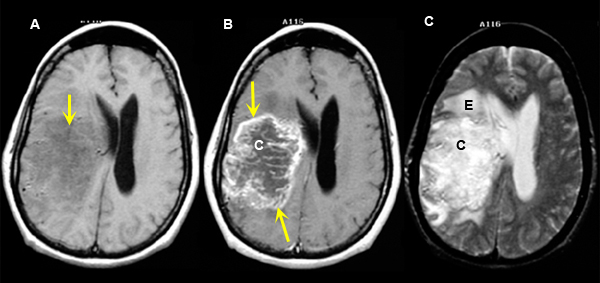 |
Figure 2 A:
Pre-contrast axial T1 wtd. MRI |
Glioblastoma
Case 2:
Imaging findings: Figure 2
- Non-specific abnormality within the right deep frontal lobe (arrow) with mass effect upon the right lateral ventricle is noted on pre contrast T1 wtd. image (fig. A.)
- Tumor demonstrates irregular peripheral enhancement (yellow arrows) with central area of cystic necrosis (C in fig. B).
- Edema (E) / cystic necrosis is visible as an area of bright signal intensity on T2 wtd. image.
Final impression:
Classic right deep frontal lobe glioblastoma demonstrating irregular peripheral ring enhancement with central area of cystic necrosis and surrounding edema.
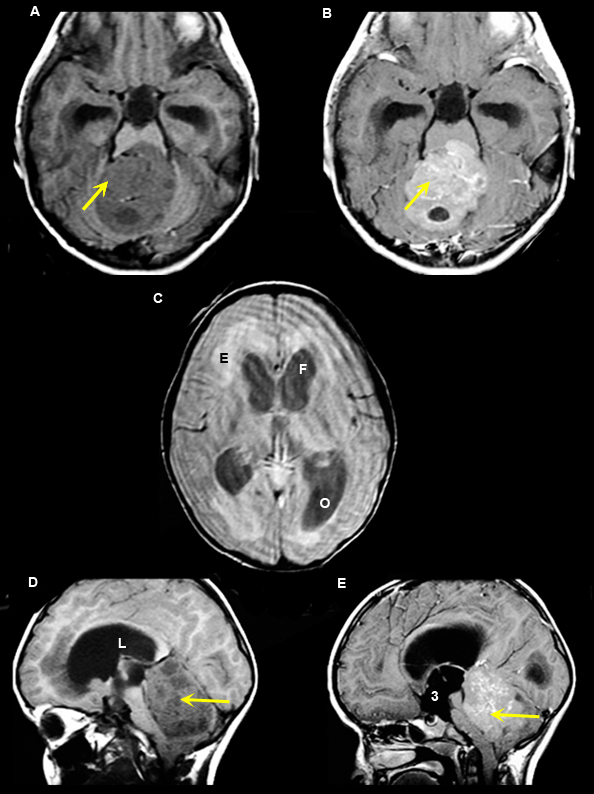 |
Figure 3 A. Pre-contrast axial T1 wtd. MRI |
Medulloblastoma
Case 3:
10 year old boy with papilledema resulting from obstructive hydrocephalus.
Imaging findings: Figure 3
- Intensely enhancing tumor (yellow arrows in figs B, E) is seen involving the roof of fourth ventricle, particularly involving the adjacent vermis.
- Obstructive hydrocephalus from medulloblastoma is noted with marked enlargement of lateral ventricles [frontal horns (F in fig. C), occipital horns (O in fi.g C), lateral ventricle (L in fig. D) and third ventricle (3 in fig. E)].
- Figs. A, D: Pre-contrast MR images show non-specific mass with hydrocephalus.
- Figs. B, E: Post-contrast MR images demonstrate enhancing characteristics of the tumor along the roof of fourth ventricle (arrows).
- Fig. C: T2 wtd. flair image demonstrates hydrocephalus involving the lateral ventricles resulting in periventricular edema (E in fig. C).
Final impression:
Medulloblastoma
Medulloblastoma is a malignant primary brain tumor originating from the roof of fourth ventricle. Most common in children and young adults. Tumor, because of its location, compresses the fourth ventricle and causes hydrocephalus. Symptoms are primarily secondary to increased intracranial pressure from hydrocephalus.
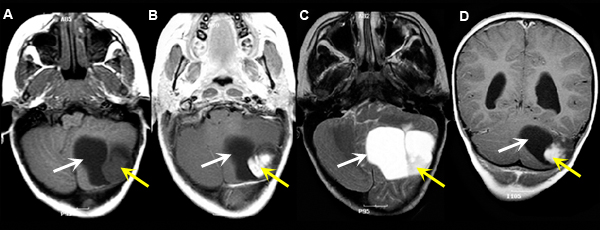 |
Figure 4 A: Pre-contrast axial T1 wtd. MRI |
Pilocytic astrocytoma (Grade I Astrocytoma)
Case 4:
Imaging findings: Figure 4
-
Left cerebellar hemispheric Pilocytic Astrocytoma with an enhancing mural nodule (yellow arrow in figs B, D) and a cystic component (white arrow).
-
White arrow in all the images points to the cystic component and yellow arrow to the mural nodule.
Final impression:
Pilocystic Astrocytoma
Pilocystic Astrocytoma is a primary brain neoplasm occurs most often in children and young adults. It is a slow growing tumor with a solid and cystic component. The solid component is well circumscribed and enhances with contrast.
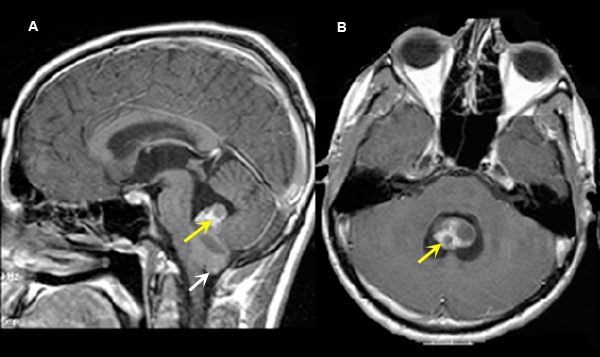 |
Figure 5 A: Post-contrast sagittal T1 wtd. MRI |
Ependymoma
Case 5:
Imaging findings: Figure 5
- Enhancing tumor (yellow arrow) is seen within the inferior portion of IV ventricle with tonsillar herniation (white arrow).
Ependymoma
Ependymoma is a glial tumor that arises from the ependymal lining of the ventricles. Location of the tumor result in obstructive hydrocephalus. Ependymoma occur within the fourth ventricle, third ventricle and lateral ventricle, more common within the fourth ventricle. Ependymoma is more commonly seen in children than adults. However, spinal cord ependymoma is seen more in adults.
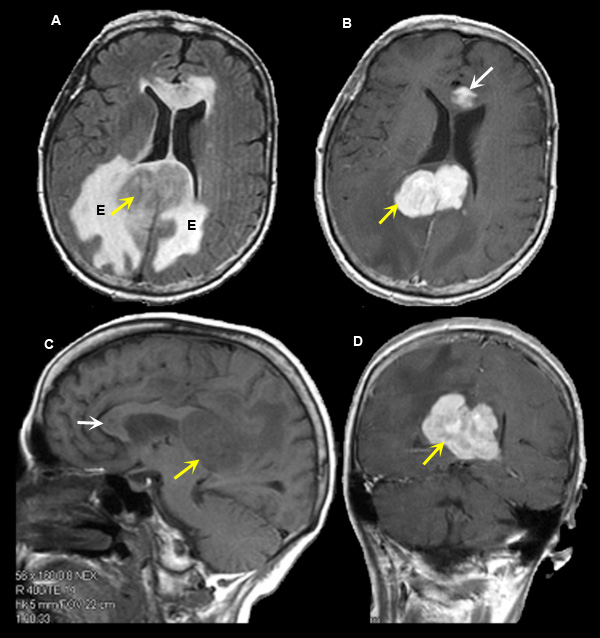 |
Figure 6 A. Axial flair image |
Lymphoma
Case 6:
Imaging findings: Figure 6
- Intensely enhancing tumor is seen involving the posterior body of corpus callosum (yellow arrow in figs B, D), including smaller tumor involving the genu of corpus callosum (white arrow in fig. B).
- Tumoral edema (E in fig. A) surrounding the lymphoma is well appreciated on axial flair image as an area of bright signal intensity.
- Non-specific abnormality is seen in the pre-contrast sagittal T1 wtd. image (fig. C).
Final impression:
Lymphoma of the posterior body of corpus callosum.
Primary brain lymphoma often occurs in immunocompromised host. Common sites of involvement include corpus callosum, basal ganglion, thalamus and periventricular white matter.