Definition
Bronchogenic carcinoma is a malignant neoplasm of the lung arising from the
epithelium of the bronchus or bronchiole.
Incidence
Accounts for 14% of all new cancers in males and 13% of
all new cancers in females.
Seventy percent of all lung cancer deaths occur between the ages of 55
and 74. However, recent trends indicate that both the incidence and mortality of
lung cancer is increasing in younger age groups.
It is approximately three times more common in men than females. However the
incidence of lung cancer in females in increasing in epidemic proportions.
Lung cancer leads as cause of cancer deaths among women and
men.
The countries with the highest incidence of lung cancer among males is the
United Kingdom
In general, the incidence of lung cancer in industrialized western countries is
increased compared to third world countries.
The highest incidence of lung cancer in the United states is in the northern
urban areas and along the gulf and south Atlantic Coasts from Texas
to Florida.
Etiology
- Smoking
- Today, the epidemiology of lung cancer is the epidemiology of smoking. Other
factors are relatively of minor importance.
- Carcinogens
- Cigarette smoke contains a number of proven carcinogens in both the particulate
and gaseous phase including:
-Aromatic Hydrocarbons
-Nitrosamines
-Nitrosonormicotine
-Polonium
-Arsenic
- Synergic
- Exposure to certain substances have a synergic effect in being causatively
associated with the use of tobacco products in development of lung cancer.
-Asbestos
-Chloromethyl Ethers
-Mustard Gas
-Radioactive Ore
- Host Factors
- As with most illnesses, the development of disease depends on a complex
interaction between the environment and the host. Specifically with lung cancer, host
factors play a relatively minor role.
-Risk of Second Primary
-Associated Malignancies
-CLL
-Aryl Hydrocarbon Hydroxylase
-Scar Carcinoma
-Tuberculosis
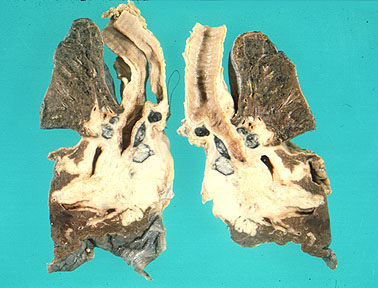
Pathology
Bronchogenic carcinomas begin as a small focus of atypical epithelial cells within the
bronchial mucosa. As the lesion progresses, the atypia becomes frankly malignant and the
neoplasm grows in size. The neoplasm may grow into the bronchial lumen, along the mucosa
or into the bronchial wall and
adjacent lung parenchyma. Eventually the neoplasm spreads to regional lymph nodes and distant organs such as the
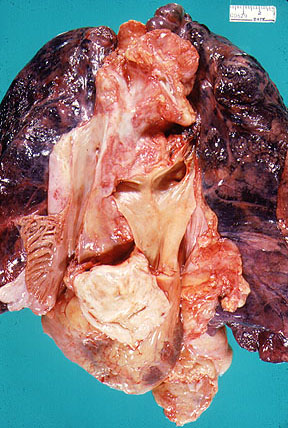
liver, brain and bone. Most bronchogenic carcinomas form a mass in or near the hilus. Some neoplasms,
especially the adenocarcinomas, form a mass in the periphery of the lung. Refer to Figure
15-42 in your textbook. The following classification scheme represents the major
histologic types of bronchogenic carcinoma. Refer to Table
15-10 in your textbook.
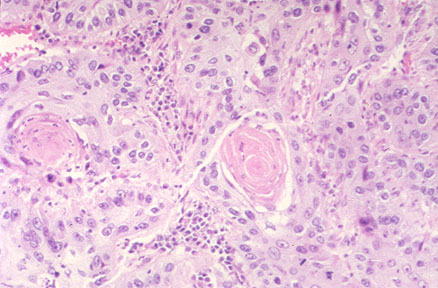
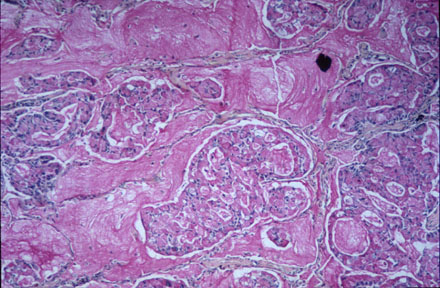
- Squamous Cell
Carcinoma: The neoplasm is composed of malignant squamous cells which may
vary in degree of differentiation from tumor to tumor. A well differentiated squamous cell
carcinoma may form keratin and intercellular bridges. . Squamous Cell Cancer: most
strongly associated with smoking, can be well, moderately or poorly differentiated. The tumor cells are large, with
pink cytoplasm and keratinization, forming keratin pearls. In the poorly differentiated
carcinomas, the cells are highly atypical with rare individual cell keratinization
CLINICAL NOTE: This neoplasm is most common in men and is closely related to
smoking.
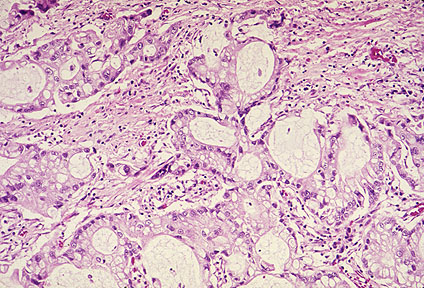
- Adenocarcinoma: Adenocarcinoma is the most common lung cancer
which usually arises from peripheral small bronchi and is often associated with a scar.
Adenocarcinomas tend to be smaller than other bronchogenic carcinomas and located in the
periphery of the lung. The tumor
cells form glands and secrete mucin. Mucus stains bright pink
with mucicarmine stain and PAS after diastase The neoplasm is composed of malignant
glandular epithelium which may vary in degree of differentiation from tumor to tumor. Well
differentiated neoplasms may form distinct glands, other neoplasms may vary from forming
papillary structures to solid neoplasms without any gland
formation.
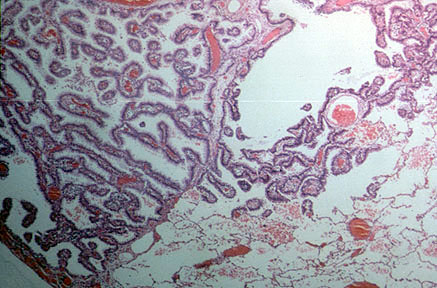
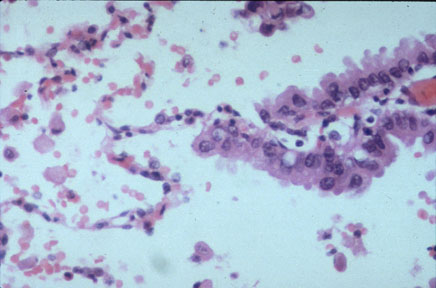
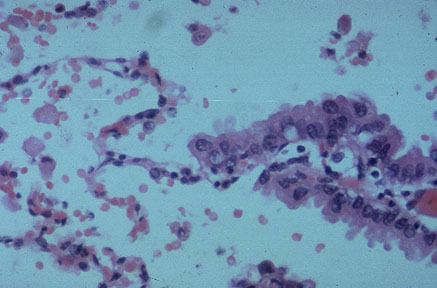
- A distinctive type of adenocarcinoma is bronchioloalveolar carcinoma.
Bronchioloalveolar carcinoma (BAC) classically spreads in a single layer on
top of alveolar septa that serve as scaffolding for the malignant cell growth. In half the
tumors the cells are tall, well-differentiated, mucin-producing with basally located
nuclei. Nonmucinous BAC is composed of tall columnar cells or cuboidal cells growing along
the alveolar walls . Bronchioloalveolar carcinoma: The neoplasm is a
distinctive form of adenocarcinoma. The neoplasm arises from the epithelium of the
terminal bronchiole or the alveolus.
The neoplastic cells are columnar, lining alveoli or form
palliary growths which project into the alveolus. The neoplasm, almost always
arising in the periphery, is solitary or forms multiple coalescing nodules.
CLINICAL NOTE: This neoplasm is the most common type in women and nonsmokers.
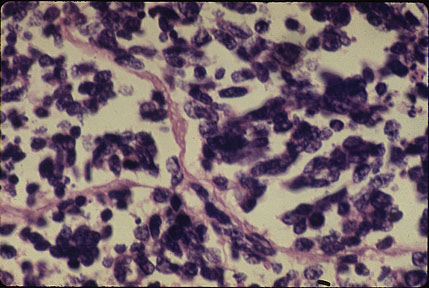
- Small cell
carcinoma: Small cell carcinoma, regardless of histologic subtype, lacks a
defined architectural pattern. It is composed of sheets of haphazardly arranged small
cells with scantly cytoplasm. At low power, the tumor appears blue due to the closely
opposed nuclei. There are numerous mitotic figures and foci of necrosis are present
The neoplasm is composed of small
cells containing dark blue, round nuclei and sparse cytoplasm. These cells resemble
(but are not) lymphocytes and are arranged in clusters. Electron microscopy reveals
that these cells contain neurosecretory granules, indicating their origin from
neuroendocrine cells. . CLINICAL NOTE: This neoplasm is strongly related to smoking. It is
a very aggressive neoplasm, generally having metastasized at the time of diagnosis.
- Large cell carcinoma: The neoplasm is composed
of large, undifferentiated malignant cells.
Pathophysiology
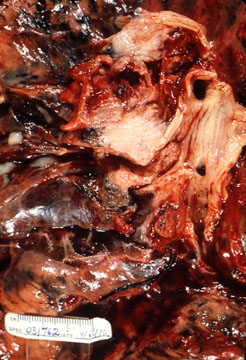
- Bronchogenic carcinoma tends to form an intraluminal mass which may partially or completely obstruct the bronchus.
The neoplasm also may compress or invade local structures such as aorta, esophagus,
superior vena cava or cervical sympathetic chain.
- Bronchogenic carcinoma may present with a variety clinical manifestations but the
major findings are cough, weight loss, chest pain and dyspnea. These neoplasms also have
the capacity to secrete hormones or hormone-like substances which have a variety of
clinical effects.
Natural History
Pre-Detectable
- Beginning with its biological onset (the development of the first frankly
malignant cell) and beginning when the disease may first be shown to exist whether through
sputum cytology or chest radiography.
- It has been claimed that by the time a tumor is 10 mm in diameter it has already
doubled in size 30 times, contains at least one billion cells, and has completed
three-fourths of its anticipated existence.
It is likely that during the majority of a lung tumor's existence it will be
undetectable by any currently available diagnostic technique.
Detectable-Asymptomatic
- Presence of the disease is potentially demonstrable, yet continues to be without
symptoms. The disease is detectable if:
- The tumor is radiographically evident (5-10 mm in diameter),
- or Sputum is positive for malignant cells.
The duration of this "presymptomstic-detectable" phase is heavily
dependent on the cell type involved and on location of the primary tumor. Sputum cytology
can be positive for several years before symptoms occur in a progress from undetectable to
unresectable within a few short months. Unfortunately, only about 5% of lung cancer
diagnoses are made in this phase. These findings are typically made through incidental
X-Ray findings during workup of an unrelated condition of through sputum and X-Ray
screening of high-risk patients.
Symptomatic Phase
About 95% of all lung cancer diagnoses are made during the phase when the
disease has become symptomatic. Carcinoma discovered at this point in its natural history
is almost always well advanced. With very few but significant exceptions, symptomatic lung
cancer carries poor prognosis. This is because the vast
majority of symptoms in this disease are caused by either locally unresectable or
metastatic tumor.
Symptoms Grouping
- Primary Tumor
:Endobronchial location of the tumor explains many of the symptoms related to primary
tumor. If the primary is peripheral and the lesion is in the lung, often the symptoms
related to primary tumor are absent.
- Cough
- Dyspnea
- Hemoptysis
- Pso-obstructive Pneumonia
- Increase in Sputum
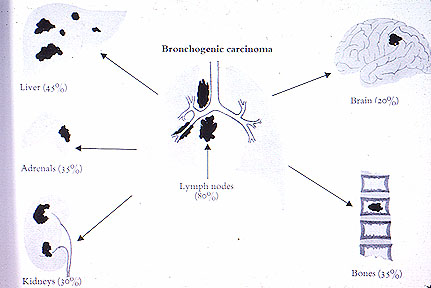
- Distant Metastasis :
Several organs or organ systems clearly emerge as the most common sites of distant
metastasis for lung carcinoma. These have great bearing on the clinical manifestations of
the disease, and are frequently the cause of the clinical manifestations of the disease,
and are frequently the cause of the patient's initial presentation!
- Brain
- Liver
- Bone
- Skin
- Adrenals
- Lymph Node
- Paraneoplastic Syndromes :
These are an ever-expanding set of intriguing clinical syndromes involving non-metastatic
systemic effects which have been noticed to accompany malignant disease on occasion. Some
are associated with a specific cell type; others have no such predilection. Most are felt
to be biochemically mediated. Some are just plain mysteries.
- Endocrine
- Musculoskeletal/Cutaneous
- Hematologic
- Neuromuscular
- Cardiovascular Miscellaneous
- Hypertrophic
Osteoarthropathy
- Clubbing
- Acanthosis Nigricans
- Thrombophlebitis
- ACTH
- ADH
- Hypercalcemia
- Intrathoracic Spread : When
carcinoma of the lung causes symptoms though intrathoracic spread, it tends to do so in
only two primary ways:
- By Contiguity
- Nodal Metastasis
Whatever the mode of spread, most of the associated symptoms occur once the
disease has reached either the chest wall or the mediastinum. If it was central,
mediastinal problems tend to occur. If the tumor was located very inferior, diaphragmatic
symptoms may be expected. If it began out in the periphery, chest wall problems are
usually noted first.
Clinical problems that result from extension to the chest wall aren't difficult
to understand. Since the parietal pleura is one of the few pain-sensitive structures in
the area, this may be the first time the patient experiences pain. Pleural effusion is
also a common condition related to this process. If the tumor happened to start near the
apex of the lung, a syndrome knows as "Pancoast Tumor" may develop, involving
complaints related to damage of CB-T1 roots.
- Non-Specific : The
following are non-specific symptoms due to tumor burden:
- Weight loss
- Malaise
- Loss of appetite
Staging
During the past years, numerous investigators have been endeavoring to establish
a standard terminology that would accurately describe the extent of a cancer. One such
staging system for lung cancer has been formulated by the Task Force on Lung Cancer of the
American Joint Committee for Cancer Staging and End-Results Reporting (AJCF). The AJC
staging system employs the T-N-M nomenclature . In this system, the letter T represents
the primary tumor N regional node involvement, M.
- T. Numerical Suffix Assignment
- The criteria are:
- Size
- Proximity to Carina
- Extent of Collapse
- Invasion of surrounding structures
- N Numerical Suffix Assignment
- The first station lymph nodes are the intrapulmonary, peribronchial and hilar
lymph nodes, which are contained within the visceral reflections. Second station lymph
nodes are those in the mediastinum and may be paraesophageal, subcarinal, paratracheal,
aortic or retrotracheal. Involvement of scalene, contra-lateral or extra-thoracic nodes is
considered distant metastasis.
-
- M Suffix Assignment
- The metastatic status is signified by the letter "M" with subscripts O
or 1 to indicate absence or presence of metastatic disease. "M1" signifies
presence of metastasis in one or more distant organs. The common metastatic sites are
Brain, Bone, Liver, Adrenal glands and subcutaneous tissue.
-
- Group Staging
- T, N and M combinations are used to group stage lung cancer. The staging is
important in planning therapy and for estimating prognosis.
Principles of Therapy
Therapeutic options consist of:
- Surgery
- Non-small cell cancer in stages 1, 2, 3a in acceptable general condition as a
surgical candidate are best suited for this modality. In general, small cell cancer is not
a surgical disease.
-
- Radiation Therapy
- If the general condition precludes the patient from being a surgical candidate,
Radiation therapy is chosen. Palliative Radiation therapy has an important role for relief
of symptoms in inoperable cases.
-
- Chemotherapy
- Chemotherapy is the treatment of choice for small cell cancer. Its role in NSCC
is under investigation.
-
- Supportive Care
One needs to consider the following in to determine the best option.
- Cell type
- Stage
- Clinical status
Prevention
Lung cancer is a preventable disease. If cigarette consumption is stopped, we
can probably prevent 99% of lung cancers. As a physician, it is your obligation to set an
example by not smoking and to advise patients not to smoke. You can offer options to aid
patients in quitting their habit.
- Nicotine chewing gum or patches
- Clinics which specialize in helping patients quit smoking
- Hypnotherapy
Take an active role in bringing legislation to curb the use of cigarettes in
public places. Additionally, advertisements should be discontinued which encourage
children to start the habit. We probably should not attempt to ban cigarettes completely.
It is unlikely to succeed, as we have learned from our past experience in trying to ban
alcohol.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}