Definition
Pulmonary tuberculosis is an infection (inflammation) caused by
mycobacterium tuberculosis.
General Introduction
Human tuberculosis is caused by M. tuberculosis and M.bovis. Both organisms share one unique characteristics (acid fastness), but only the former can be cultured on artificial media.
Mycobacteria are uniquely capable of surviving within macrophages, and macrophages have to be activated in order to kill the intracellularly residing tubercle bacilli.
Tuberculosis and other mycobacterial infections (excluding leprosy) are becoming increasingly prevalent among compromised hosts, especially AIDS patients.
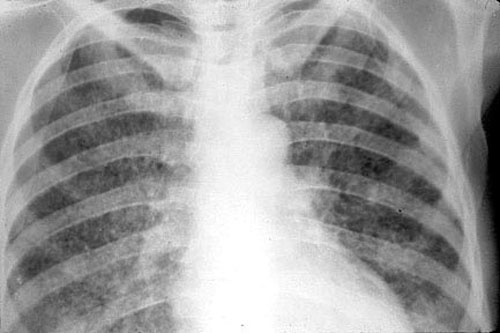
In man, the lungs are most commonly affected, but lesions may occur also in the kidneys, bones, lymph nodes, and meninges or be disseminated throughout the body.
Characteristics of the Etiological Agents
The route of infection (respiratory versus intestinal) determines the pattern of lesions.
In developed countries, M. bovis has become very rare.
Some "atypical" mycobacteria (e.g., Mycobacterium fortuitum) cause (see nontuberculous mycobacterial infections in compromised hosts).
| Pathogenicity of Mycobacteria | |||||
|---|---|---|---|---|---|
| Species | Human | Guinea Pig | Fowl | Cattle | Cause TB |
| M.tuberculosis | +++ | +++ | - | - | Yes |
| M.Bovis | +++ | +++ | - | +++ | Yes |
| M.Kansasii | +++ | - | - | - | No |
| M.avium-intracellulare* | + | - | +++ | - | No |
| M.fortuitum-chelonei* | + | - | - | - | No |
Microbiological Characteristics
Obligate Aerobic
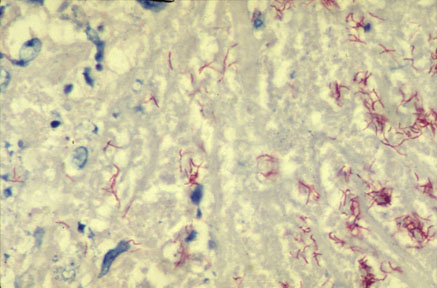
Acid-Fastness (For Mycobacteria, Gram Positiveness is Only Academic)
Special Nutritional Requirement (Lowenstein-Jensen Medium)
Slow Grower
Highly Resistent to Desiccation
Facultative Intracellular Pathogen
Unique Cellular Constituents (Lipids)
Pathogenesis of Tuberculosis
Inhalation: Contaminated Dusts or Droplets
Ingestion: Contaminated Milk (Uncommon in the Western World) - Tuberculosis Due to M. Bovis.
Spread, Multiplication and Damage
Cellular Components of M. Tuberculosis Contributing to the Pathogenesis
Lipids
Mycobacteria are rich in lipids. Phosphatide fractions can produce tubercle like cellular
responses and caseation necrosis. Lipids are to some extent responsible for acid-fastness.
Virulent strains of tubercle bacilli form microscopic "serpentine cords" in
which acid-fast bacilli are arranged in parallel chains. Cord formation is correlated with
virulence. A "cord factor" (trehalose-6,6'-dimycolate) has been extracted from
virulent bacilli with petroleum ether. It inhibits migration of leukocytes, causes chronic
granulomas, and can serve as an immunologic "adjuvant".
Proteins
Each type of mycobacterium contains several proteins that elicit the tuberculin reaction.
Proteins bound to a wax fraction can, upon injection, induce tuberculin sensitivity. They
can also elicit the formation of a variety of antibodies.
Polysaccharides
Mycobacteria contain a variety of polysaccharides. They can induce the immediate type of
hypersensitivity (clinically not relevant).
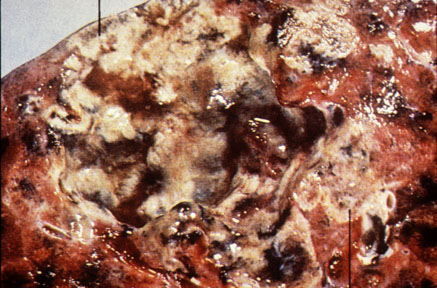
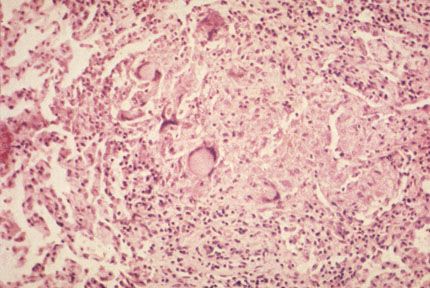
Pathology
The characteristic pathologic changes depend on the type of infection or
"exposure." If the primary lesion could not contained rapidly, the appearance of
hypersensitivity to tuberculin (see below) provokes a dramatic change in the host's
response to the organisms. The nonspecific inflammatory response evoked on first exposure
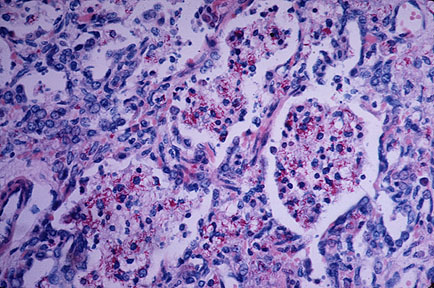
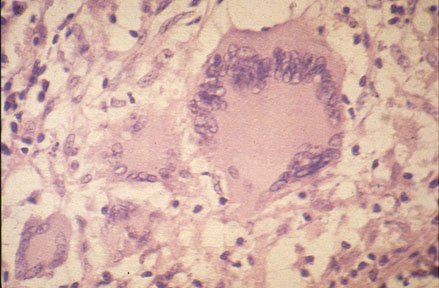
to tubercle bacilli becomes granulomatous, evoking the formation of tubercles. The
tubercle comprises an organized aggregation of enlarged macrophages that, because they
resemble epithelial cells, are referred to as epithelioid cells. A peripheral collar of
fibroblasts, macrophages, and lymphocytes surrounds the granuloma. Frequently the central
region of epithelioid cells undergoes a characteristic caseous necrosis to produce a
"soft" tubercle, the most characteristic hallmark of tuberculosis. When the
antigen load at the initial infection site and regional lymph node is large, caseation
necrosis may develop and lesions may later calcify.
Primary Tuberculosis
When the host encounters with M. tuberculosis for the first time, the following events occur:
As illustrated above, when a host has first contact with tubercle bacilli:
Progressive primary infection:
After the development of hypersensitivity, the infection becomes quiescent and asymptomatic in the majority of patients (about 90%). In some, however, especially the very young and adults who are immunocompromised or who have other predisposing illnesses, the primary infection may evolve into clinical disease. The progression may be local at the site of the primary lesion, or it may be at one or more distant sites where bacilli have arrived during the early hematogenous spread.
Secondary or Reactivated Tuberculosis
In a small number of persons whose initial tuberculous infection subsidies, secondary disease occurs in spite of acquired cellular immunity.
Secondary tuberculosis is usually due to the reactivation of old lesions.
The characteristics of secondary tuberculosis include extensive tissue damages due to immunologic reactions of the host to tubercle bacilli and their products.
In this phase of the disease, lesions are usually localized in the apices of the lungs (remember that tubercle bacilli require oxygen for growth).
In about 5% of patients, apical pulmonary tuberculosis manifests itself within 2 years of the primary infection. In others, however, clinical disease may evolve many decades later whenever resistance is lowered.
Quiescent foci that harbor viable organisms thus remain a potential hazard throughout a person's lifetime.
Because of the acquired cellular immunity, bacilli are more promptly phagocytized and destroyed by the activated macrophages. As a result, in secondary tuberculosis, lesions remain localized and dissemination of organisms via the lymphatic vessels is usually prevented.
Hypersensitivity promotes a more rapid caseation and fibrotic walling-off of the focus. Histologically the reaction is characteristic of tubercle formation, manifested by a local accumulation of lymphocytes and macrophages.
T lymphocytes and their chemotactic lymphokines play a major role in the development of tuberculous granuloma.
These differences between primary infection and post-primary or reactivation are attributed to (1) resistance and (2) hypersensitivity induced by the first infection of the host with tubercle bacilli.
Therapy:
References: Sherris Medical Microbiology, Chapter 27
Last Updated: January 13, 2000 Created: March 14, 1996
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}