Chronic myelogenous leukemia
Chronic myelogenous leukemia (CML) accounts for approximately 15 to 20 percent of cases of leukemia in adults. The median age at presentation is about 50 years of age. Exposure to ionizing radiation is the only known risk factor. CML has a chronic phase, which is present at the time of diagnosis in most patients, an accelerated phase, in which neutrophil differentiation becomes progressively hindered and myelosuppressive medications fail to effectively control leukocyte counts, and blast crisis, an acute leukemia-like condition in which myeloid or lymphoid blasts fail to differentiate. Up to 50 percent of initially diagnosed patients are asymptomatic, with the disease first being suspected from routine blood tests. Those with symptoms may present with fatigue, malaise, weight loss, excessive sweating, abdominal fullness, and bleeding episodes due to platelet dysfunction. Splenomegaly, anemia, and elevated white blood cell count are common.
he diagnosis of CML is typically established by demonstration of the Philadelphia chromosome or the BCR-ABL fusion gene. Specifically, the chromosome abnormality involves an exchange of material between chromosomes 9 and 22 (Figure 1). 95% of patients with CML show this abnormality. The result is that part of the BCR gene from chromosome 22 (region q11) is fused with part of the ABL gene on chromosome 9 (region q34) (Figure 2). The BCR-ABL fusion protein, which is constitutively active, activates cell cycle-controlling proteins, accelerating cell division. It also inhibits DNA repair, causing genomic instability and potentially causing blast crisis. In the late 1990s, a medicine called Imatinib (Gleevec) was identified as a powerful tyrosine kinase inhibitor that can combat CML by binding to the ATP binding site of BCR-ABL (Figure 3). Some forms of CML are resistant to Imatinib.
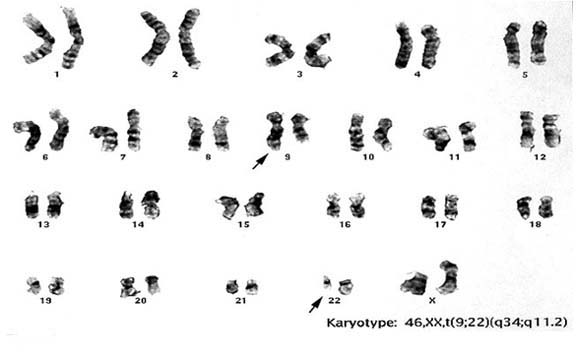
Figure 1.
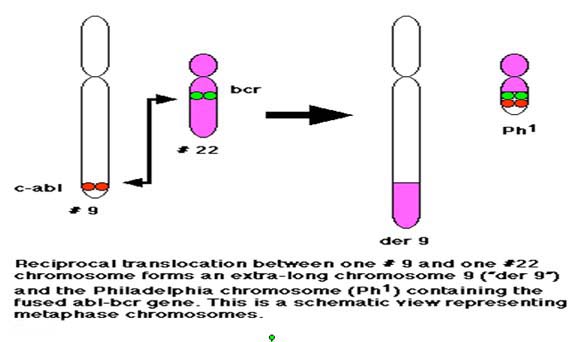
Figure 2.
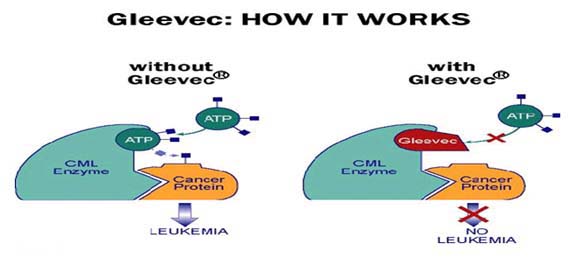
Figure 3.
A 50 year old male presents with fatigue, malaise, and abdominal fullness. Clinical evaluation shows splenomegaly, anemia, and elevated white blood cell count. You suspect he might have CML.
- Which laboratory test would be most important in confirming a diagnosis of CML?
- What might be one potential cause for Imatinib resistance?
- Cytogenetic studies show that the patient does carry the Philadelphia chromosome in his blood. What is the chance that his children have inherited this translocation?