Drainage Areas
The SVC is the major trunk line for return of venous blood to the right heart from the:
The knowledge of the anatomic drainage of the SVC helps you to understand the clinical manifestations of this disorder.
Once the superior vena cava is compromised, a magnificent collateral system begins shouldering the burden of returning venous blood to the right heart from the head, neck, upper extremities and upper thorax. The efficiency of the collateral circulation determines the patients comfort, degree of disability and prognosis. A superior venocavogram demonstrates these collaterals.
The major collateral channels are:
Azygous and Hemi-Azygous
The azygous and hemi-azygous systems are the major routes for diversion of blood flow. These dilated vessels often widen the mediastinum on CXR and can be mistakenly interpreted to represent mass lesions.
When the obstruction is above the azygous vein, this major axillary channel takes over the function of the SVC.
When the obstruction occurs below the azygous arch or includes it, the patient tolerates this with far more difficulty. The venous pressure is much higher and the immediate prognosis more serious. The route of venous blood flow is now much more circuitous and complex and involves the support of the inferior vena cava.
For a comprehensive review of collaterals, refer to:
References:
Physical Findings
Edema of Upper Body
The upper body manifests signs of edema because its major flow of venous return is
obstructed, as compared to the lower body which is drained by the unobstructed inferior
vena cava.
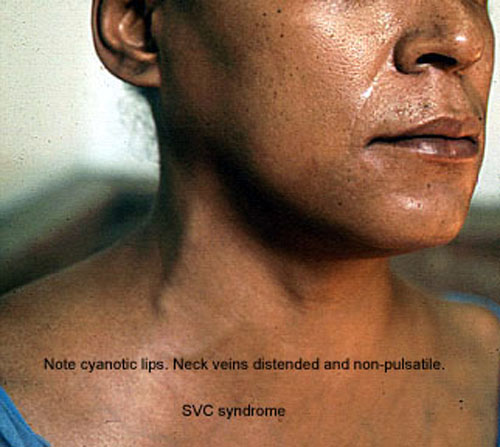
Cyanosis
Due to the local stagnation of blood flow and subsequent oxygen extraction, there is
described "preferential" cyanosis. This is distributed to the face, neck and
upper extremities.
Plethora
There is plethora of the upper body due to the combination of cyanosis and hyperemia of
distended vessels.
Collateral Distention
Once the flow in the SVC or its tributaries become compromised, a complex system of
collateral veins begins to develop. These prominent veins on physical exam can be seen
along the anterior chest wall,
axilla and abdominal wall. There is reversal of blood flow
in the veins of the upper abdominal wall toward the inferior vena cava.
Capillary dilatation
In chronic SVC obstruction due to benign causes, one often sees diffuse capillary
dilatation on chest wall.
Neck Vein Distention
Neck veins are distended and
non-pulsatile in SVC syndrome as opposed to congestive heart
failure where they are pulsatile.
Veins in arms do not collapse when lifted.
Orthopnea
Patients with SVC syndrome have severe Orthopnea. Gravity helps venous return to heart in
the erect position. In supine position the venous return dramatically drops leading to
severe shortness of breath.
Findings of anterior mediastinal mass
Examine for physical findings of anterior mediastinal mass. Superior vena cava is in the
anterior mediastinum and the most common cause for SVC obstruction are Lymphoma and Lung
cancer with mediastinal nodes. Examine also for Goiter.
Caution: In SVC syndrome you may feel "hard supraclavicular node like structure". Most of the time they are distended vessels.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}