55 year old female with a history of idiopathic pulmonary fibrosis who was 4 weeks status post single lung transplantation. Her post-operative course was complicated by diffuse weakness necessitating transfer to an acute rehabilitation facility. At rehab, the patient was doing well. She had no fever, chills, change in her chronic cough or dyspnea. She was able to participate in her rehabilitation activities and was progressing as expected. On the day of admission the patient complained of acute onset of dyspnea. She was found to be tachypneic and cyanotic with a respiratory rate of 38. Exam revealed crackles on the right and diminished breath sounds on the left. She was transferred to the closest hospital where she was emergently intubated.
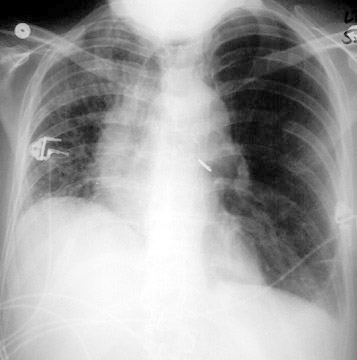
Chest x- ray findings (baseline, day of transfer).
The patient became hypotensive shortly after intubation and a continuous infusion of dopamine was started. Throughout her stay at the initial hospital the dopamine was progressively increased for persistent hypotension. A pulmonary angiogram was negative for pulmonary embolism (PAP 50/25 mm Hg) and an echo revealed normal LV and RV systolic function with no pericardial effusion. It was elected to transfer the patient to this hospital. Mechanical ventilator settings and arterial blood gases over the first several hours of her hospitalization, and during transport were as follows:
| Time | Rate | Tidal Volume | FIO2 | PEEP | pH | pCO2 | pO2 |
| 15:33 | 22 | 300 | 1.0 | 0 | 7.16 | 84 | 290 |
| 16:16 | 24 | 300 | 1.0 | 0 | 7.13 | 93 | 513 |
| 17:30 | 40 | 300 | 1.0 | 0 | 7.05 | 105 | 178 |
| 20:28 | 40 | 320 | 1.0 | 0 | 7.06 | 113 | 483 |
| 21:00 | Rapidly bagged during transport | 7.01 | |||||
On arrival at this hospital the patient was unresponsive, cyanotic and hypotensive (75/50) on 20 mcg/kg/min of dopamine with the ventilator settings above. Exam revealed crackles on the right and quiet breath sounds on the left. The peak airway pressure was 60 cm H2O, the pressure after a 1 second inspiratory pause (plateau pressure) was 50 cm H2O.
What would be your first step in the management of this patient?
The most striking finding in this patient’s hospital course is the progressive increase in arterial pCO2 in response to incremental increases in the minute ventilation. In steady state, the sole determinants of the arterial pCO2 are the
Short-term changes in carbon dioxide production are unlikely, therefore, the increasing pCO2 despite a higher minute ventilation must be caused by a progressively increasing dead space fraction.
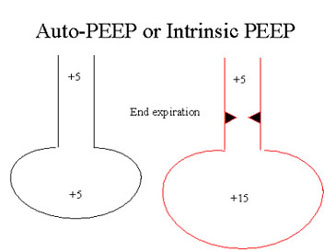
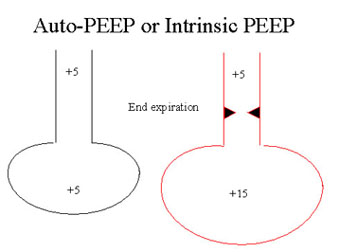
The cause of the increased dead space fraction is dynamic hyperinflation or auto-PEEP. Short expiratory times do not allow for complete emptying of the alveoli by the end of expiration. This results in alveolar pressure exceeding airway pressure at the end of expiration. Patient’s with airflow obstruction, whose expiratory times are prolonged, are particularly prone to the development of auto-PEEP .
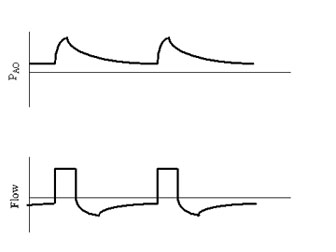
Auto-PEEP can be measured in sedated or paralyzed patients by inserting an end-expiratory pause on the ventilator . In spontaneously breathing patients on the ventilator, however, inspiratory efforts prevent auto-PEEP measurements. In these patients, auto-PEEP can be inferred by examining the flow tracing on the ventilator. The presence of expiratory flows at the beginning of inspiration confirms the presence of auto-PEEP.
Auto-PEEP can result in
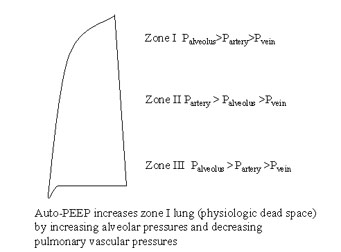
Hypotension can result from the decreased venous return associated with increased intrathroacic pressures. High levels of auto-PEEP can increase the dead space fraction by creating additional West Zone I lung due to both increased alveolar pressures and decreased pulmonary artery pressures.
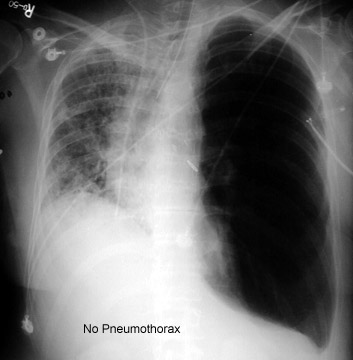
This patient had severe dynamic hyperinflation as evidenced by her hypotension, increasing dead space fraction, unilateral hyperinflation on chest x-ray and high plateau pressure on the ventilator. Shortly after arrival in the ICU her respiratory rate was decreased to 12 per minute with immediate, marked improvements in her hemodynamics and arterial pCO2 and chest x-ray(link to pre and post film). Emergent bronchoscopy revealed a mucous plug in the left mainstem bronchus at the site of anastamosis creating a ball valve obstruction. Airway pressures normalized after removal of the plug and the patient was extubated 6 hours later.
Dynamic hyperinflation or auto-PEEP should be suspected in patients with airway obstruction and hemodynamic instability. A brief (2 minute) trial of cessation or decreased minute ventilation will result in rapid improvement in hemodynamics, confirming the diagnosis. Such a maneuver may be life-saving.
References:
T. Corbridge and J.B. Hall. Status asthmaticus in J.B. Hall, G.A.Schmidt. L.D.H. Wood., Eds. Principles of critical care. McGraw Hill. New York. 1998. P. 579-595.
A.R. Leff and P.T. Schumacker. Respiratory Physiology. W.B. Saunders. Philadelphia. 1993. P. 47-69.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}