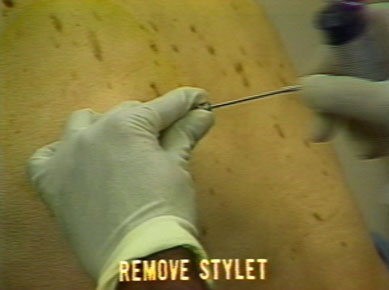
Avoid the two most common mistakes made with this maneuver. Remember to remove the two inner tubes together. Removing them singly causes confusion and facilitates the development of a pneumothorax. It is important to train the patient to make a long "ooooh" sound. Instruct him to continue doing so until you instruct him otherwise.
There will be sufficient time for exchange of a stylet to a biopsy needle. If the patient is unable to expire long enough, do the exchange in two steps; keeping the outer cannula closed with a finger tip. Are you ready for "ooooh"?
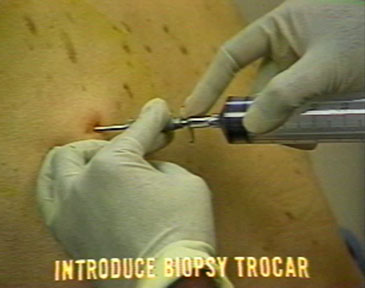
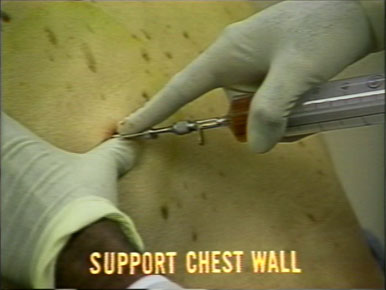
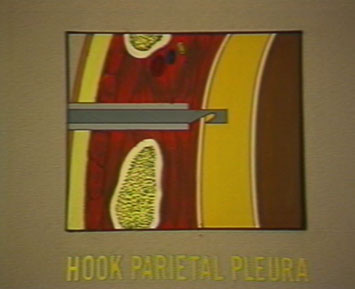
Turn the biopsy needle so that the right angled projection is facing downwards. Support the site of the chest wall with your thumb where the biopsy will be taken. Gently pull the biopsy needle as a single unit by applying downward and outward pressure until it hooks the parietal pleura. This movement should be done in one continuous motion.
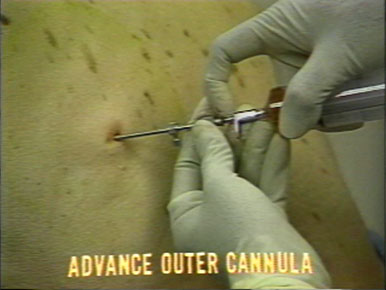
Remember to pull the outer cannula and the biopsy needle together as a single unit. Once you have hooked the pleura, hold it with gentle traction and advance the outer cannula with a rotary motion. This maneuver will cut a piece of pleural tissue and intercostal muscle for a biopsy.
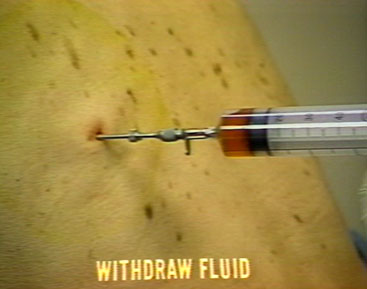
Withdraw biopsy needle: Instruct the patient to make an "ooooh" sound and remove the biopsy needle and replace the stylet. Do not be in a rush to close the outer cannula with your finger, as you are removing the biopsy needle. You may end up hooking your glove into the biopsy needle.
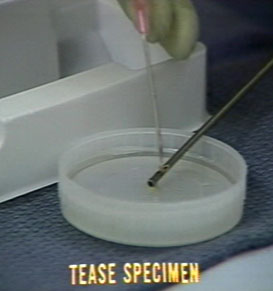
Tease the specimen out of the trocar with a needle attached to a syringe. Cover the specimen with pleural fluid to keep it moist.
Multiple biopsies: Re-introduce the biopsy needle. The pleura may be biopsied in segments along a downward directed arc of 180 degrees. Never direct the hook upwards for fear of injuring the neurovascular bundle. Repeat the biopsy procedure until four or five samples of tissue are obtained.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}