li-11-7
GRAFT-VERSUS-HOST DISEASE
by Dr. E. Orfei
DEFINITION
Clinical syndrome
following allograft bone marrow transplantation or following blood transfusion
with non-irradiated blood in an immunosuppressed patient.
The reaction may
develop in two forms: as an acute reaction within 6 weeks from
marrow transplantation or as a chronic reaction developing between100 and
400 days after transplantation. The chronic form may affect individuals who
survived the acute form or can attack de novo. The difference between the two
forms is not only in the different time of onset but also in the difference of
the organs affected. The acute form involves mainly skin, gastro-intestinal
tract and liver. The chronic form produces a disease similar to an
autoimmune syndrome involving multiple organs: liver, skin, intestine, lachrymal
glands, salivary glands and other organs.
The acute form is
probably caused by immunocompetent cytotoxic lymphocytes attacking the tissues
of the recipient thus it does not responding cyclosporin treatment.
The chronic form seems
to be caused by an immune disorder and responds to cyclosporin.
The acute form
carries a 50% mortality. The chronic form, especially when develops after the
acute phase is also equally fatal. The patients don’t die of liver failure but
because of superimposed infections.
The diagnosis
is made mostly on clinical manifestations . Only in doubtful cases liver biopsy
is required in order to recognize DVHD from other liver injuries such as radiation,
immunosuppressant drugs and opportunistic infections .
ACUTE
FORM
CLINICAL
MANIFESTATIONS
Skin rash diarrhea
and jaundice is the complete clinical manifestation of the disease, appearing altogether
or isolated in variable intensity. There are no signs of liver
failure such as ascites and encephalopathy. Abnormal liver function tests
usually precede the onset of jaundice. Cases of normal alkaline phosphatase but
with positive biopsy have occurred.
PATHOLOGY
Laboratory Tests:
-serum alkaline
phosphatase: usually increased, but may be normal.
-bilirubin,
increased.
-transaminases
moderately elevated
-anti-mitochondria
antibodies, present in a minority of cases.
Liver biopsy:
-lobular
inflammation: focal with liver cell necrosis with lymphocitic infiltration
and eosinophilic bodies. Seen in 50% of cases
-cholestasis:
canalicular and prominent, present in about all cases
-Kupffer cells:
proliferated with erythrophagocytosis and hemosiderosis.
-Portal
inflammation: is minimal with sparse cytotoxic lynphocytes.
-Interlobular bile
ducts: damage consisting of epithelial swelling, picknosis and necrosis, rupture
of the wall and lymphocytes attacking ductal cells. Ductal
damage is the most consistent damage.
-Periportal area: clean.
-Fibrosis:
none.
-Endothelialitis
consisting of attachment of lymphocytes to the endothelium o f central a portal
veins. This change is considered specific for GVHD by some authors.
CHRONIC
FORM
The
chronic form is a multiorgan autoimmune-like disease and is treated like an
autoimmune disease.
In
most cases it is preceded by the acute form. About 30% are de novo
onset. It appears between 100 and 400 days after the bone marrow
transplantation. The organs affected are skin, intestine lachrymal glands ,
salivary glands, mouth and other organs. The liver is involved in about 90% of
cases. In this form , cholestasis may be more severe than in the acute form.
Alkaline phosphatase my reach levels of 30 times normal. Jaundice may affect 50%
of cases and may sometimes severe. There is moderate increase of serum
transaminases. Anti mitochondrial and anti liver/kidney may be found.
The liver
biopsy will show severe bile duct damage with disappearance of their lumen.
Portal and lobular inflammation may be slight or very severe. There may be seen
periportal fibrosis. Cirhhosis is a rare complication.
ILLUSTRATIONS
Click
on the pictures to enlarge
 Fig,
11-7-1. Organs involved.
Organs affected by
GVHD
after bone marrow transplant and after non-irradiated blood transfusion
in
a immunosuppressed patient.
where
also the bone marrow is affected with severe aplasia. |
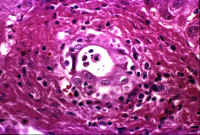
Fig.11-7-2.
Bile duct damage.
The
epithelium and wall are damaged and infiltrated by lymphocytes which are
relatively few and T type. |
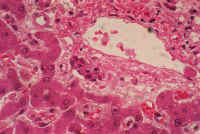 Fig.11-7-3.Disappearingduct.
Fig.11-7-3.Disappearingduct.
The
nuclei are picknotic . The
lumen
has disappeared. Notice the scarcity of inflammatory cells.
|
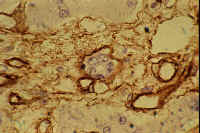 Fig11-7-4.Cytotoxic damage. Interlobular bile duct attacked by a lymohocyte in
acute form of GVHD
Fig11-7-4.Cytotoxic damage. Interlobular bile duct attacked by a lymohocyte in
acute form of GVHD
|
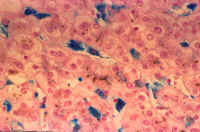
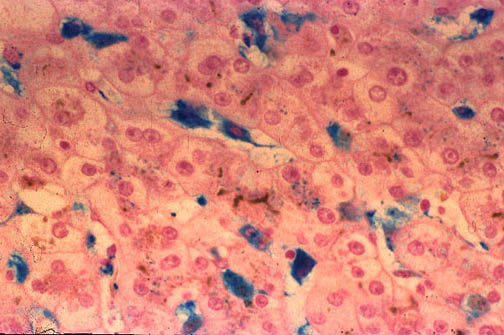
Fig.
11-7-5. Kupffer cell reaction. Marked
proliferation of Kupffer cells with siderosis
and
erythrophagia. Notice also canalicular cholestasis |
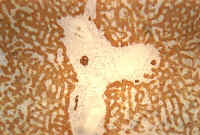
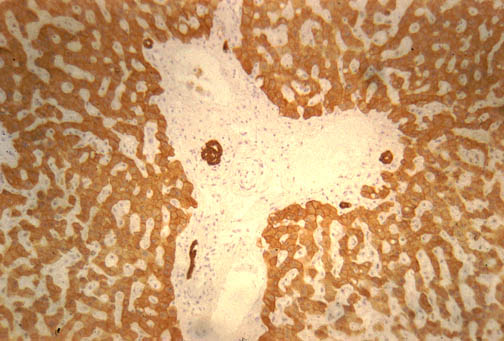
Fig. Fig.11-7-6.Ductal atrophy.
Remnants of bile ducts in a portal area. Keratin immuno- stain for bile ducts
|

Fig.11-7-7. Fig. 11-7-7. Normal
control. Portal area with normal bile ducts satained
with same compound as previous slide. |
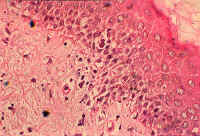 Fig.11-7-8. Skin Changes.
Fig.11-7-8. Skin Changes.
Notice the infiltration of lynphocytes of the basal
layer of the epidermis in early skin damage which can proceed to
complete sloughing of the epidermis. |
TO CONTENTS


 Fig.11-7-3.Disappearingduct.
Fig.11-7-3.Disappearingduct.
 Fig11-7-4.Cytotoxic damage. Interlobular bile duct attacked by a lymohocyte in
acute form of GVHD
Fig11-7-4.Cytotoxic damage. Interlobular bile duct attacked by a lymohocyte in
acute form of GVHD