 |
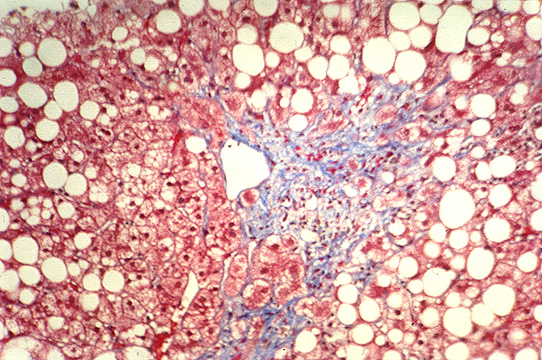
Fig.153-Alcoholic steatosis
Panlobular.Vesicles are larger
in the center of the lobule.
notice perivenular fibrosis/.
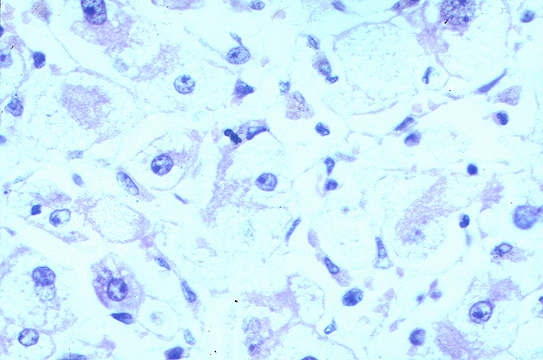 |
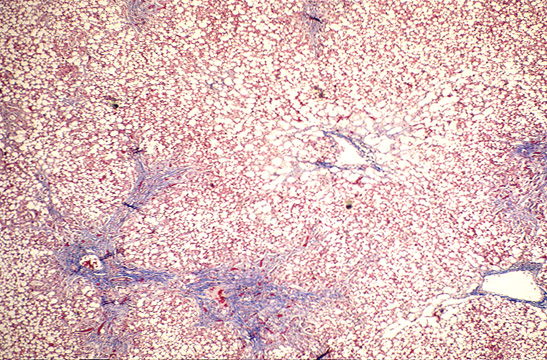
Fig.154-Alcoholic steatosis
Macrovesicular
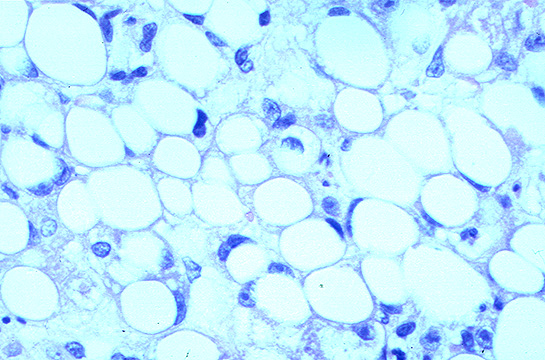 |
Fig.155-Alcoholic steatosis
Microvesicular
li-8-2
ALCOHOLIC LIVER DISEASE
Pathology
Ethanol is the chemical compound most responsible for liver damage in some parts
of the world. In the liver it causes two basic changes: 1) alcoholic fatty infiltration
and 2)alcoholic hepatitis. The latter is more severe than the former because
alcoholic hepatitis when is persistent invariably terminates in cirrhosis. The following
lesions can be morphologically recognized.
1-Alcoholic steatosis.
2-Alcoholic hepatitis.
3-Fibrosis.
4-Phlebosclerosis.
5-Cirrhosis.
6-Hepatocellular carcinoma.
7-Alcoholic siderosis.
1-ALCOHOLIC STEATOSIS
It occurs in two forms macrovesicular and microvesicular. It starts
and it is most severe in the central perivenular area but it may involve the total
surface of the lobule (panacinar).
Macrovesicular alcoholic steatosis
Presence of large sharp fat droplets in hepatocytes. The nuclei are in peripheral
location. Some vacuoles coalesce and form large cysts. There is usually minimal focal
inflammation. In some cases there may be cholestasis which may become severe and
fatal. Superimposed viral hepatitis may be the cause of these complications. Uncomplicated
fatty infiltration produces hepatomegaly but no other clinical or biochemical changes.
About 65 % of chronic heavy drinkers may develop this type of steatosis. Perivenular
central zone of the lobule is initially involved but the entire lobule may be affected
(panacinar steatosis). The accumulation of fat is attributed to a defect of secretion
of lipoprotein by the hepatocytes due to a defect of protein synthesis resulting
from interference of alcohol with assembly of tubulin into microtubules (Baraona
E. et al. J Clin Invest 60:546-54,1977). The best method to demonstrate fat is
osmium tetroxide fixation.
Microvesicular alcoholic steatosis. (Foamy steatosis)
This form of steatosis occurs more rarely and consists of groups of foamy hepatocytes
containing small fat droplets throughout the cytoplasm. The nuclei in these cells
are centrally located. There is macrovesicular steatosis, focal necrosis and cholestasis
in other areas of the same tissue but no Mallory bodies are seen. Clinically there
is jaundice and elevation of alkaline phosphatase but no fever or leukocytosis like
in alcoholic hepatitis. Microvesicular changes appear to be the first stage of hepatic
decompensation. (Uchida, Gastroenterology 84:683,1983). It will resolve without
complications with the cessation of alcohol.
Diagnosis of steatosis can be made only by liver biopsy because the liver
function tests in use are usually normal. The biopsy is performed also with the intend
to of detecting eventual complications such as fibrosis, inflammation etc.
Prognosis.Uncomplicated alcoholic fatty liver or even with minimal fibrosis will
return to normal in 4 to 6 weeks of abstension from alcohol.
Fig.153-Alcoholic steatosis Panlobular.Vesicles are larger in the center of the lobule. notice perivenular fibrosis/. |
Fig.154-Alcoholic steatosis Macrovesicular |
Fig.155-Alcoholic steatosis Microvesicular |
2-ALCOHOLIC HEPATITIS
It is a necroinflammatory lesion occurring in the centrolobular area and characterized
like any other hepatitis by necrosis, inflammation and fibrosis.
1- Necrosis is focal or confluent in the perivenular central zone of the lobule and consists of ballooning degeneration with or without Mellory bodies, giant mitochondria and, very rarely, acidophilic cells.
2- Inflammation consists of infiltrates of neutrophilic leucocytes around necrotic hepatocytes especially those containing Mellory bodies.
3-Fibrosis develops in persisting cases and may be pericellular, perivenular and bridging from central vein to an adjacent central vein according to the extent and the duration of the lesion. Lympho-histiocytic infiltrate accompanies the fibrosis. In some cases a veno-occllusive lesion of central and sublobular veins can be observed.
Mallory body formation is the result of damage and aggregation of intermediate filaments of hepatocytes.
The function of these filaments is that of maintaining the shape and the volume of the cell. Their destruction causes ballooning dilatation and cytolysis. Presence of Mallory bodies in alcoholic hepatitis is not pathognomonic but it is significant if they are seen in the central zone of the lobule.
Diagnosis of alcoholic hepatitis
is made by history and clinical and laboratory findings. The most useful biochemical
test is GGT (gamma glutamyl tranferase). Alcohol stimulates the synthesis
of this enzyme by the liver. It is however not specific for alcoholism because other
compounds (phenobarbitone, phenytoin) produce the same effect on this enzyme. Moreover
it can be low in decompensated cirrhosis and in drinkers of many years duration.
If its elevated lvel falls after one week of alcohol abstention, it is diagnostic
for alcoholism.
Prognosis of alcoholic hepatitis
In a group of patients who abstained from alcohol and were followed for 9 years with
repeated biopsies (Galambos, Gastroenterology 63:1026,1972), 27% showed normal
histology; 55% had persistence of the lesion; 18% developed cirrhosis.
3-ALCOHOLIC FIBROSIS
Fibrosis may complicate both, alcoholic fatty liver and alcoholic hepatitis.The
following forms of fibrosis with increasing severity can be observed.
Perivenular fibrosis.
Occlusive venous fibrosis
Sclerosing hyaline necrosis (massive fibrosis in central lobular area).
Fibrosis In fatty liver.
It starts in the perivenular region and extends into the sinusoids of the central
zone in a pericellular fashion forming a fine reticulum around individual hepatocytes
to assume a chicken wire configuration. The wall of the central vein becomes surrounded
by a thick layer of collagen. Fibrosis in fatty liver is not accompanied by
any sign of hepatitis. No necrosis , no inflammation , no Mallory bodies. If alcohol
consumption continues the fibrosis will increase and terminates in cirrhosis in about
20% of patients. In summary the following fibrotic patterns can be seen:
Perivenular fibrosis.
Pericellular sinusoidal fibrosis.
Chicken wire fibrosis.
These types of initial fibrosis may resolve with abstention.
The recognition of fibrous complication of fatty liver is important because it involves
a prognosis poorer than simple uncomplicated fatty liver.
Fibrosis in alcoholic hepatitis
Initially it is seen in perivenular region and in foci of necrosis. It progresses
to become pericellular and massive in the central area and may cause occlusion of
the central veins with production of portal hypertension without cirrhosis. From
necrotic areas fibrosis may become confluent and form bridging septa, central-central
and portal-central. Fibrosis is accompanied with inflammation.
The extent of necrosis and fibrosisand inflammation correlate with the progression
of the liver injury.
Fig. 156-Alcoholic fibrosis Pericellular "chicken wire" fibrosis. |
Fig. 157-Alcoholicfibrosis Centrolobular fibrosis |
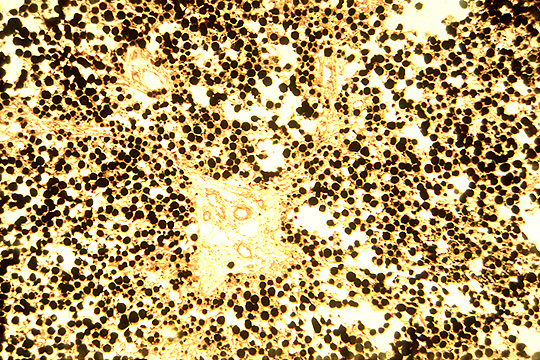
Fig.158-Alcoholic steatosis Fat globules fixed with osmium tetroxide |
Prognosis of alcoholic fibrosis.
Initial fibrosis in maro and micronodualr fatty liverwillresove with alcohol abstension.
Severe fibrosis may progress to cirrhosis even without continuation of alcohol consumption.
Factors affecting progression to cirrhosis are: continuing drinking; severity of
the initial lesion and sex, females being more affected than males.(Pares, j Hepathology
2:33,1986).
4-ALCOHOLIC CIRRHOSIS
It occurs in circa 20% of alcoholics. In people that continue to drink the cirrhosis
is micronodular and regular with 3-4 mm nodules. In people who stop drinking, the
cirrhosis may be macronodular with large dissecting nodules retaining portal tracts
and central veins and presence of wide scars and regenerative nodules. Changes of
alcoholic hepatitis and steatosis may be present. Globules of alpha-1-antitrypsin
and copper granules may be seen in hepatocytes at the periphery of regenerative nodules.
For the evolution and complications of cirrhosis consult the chapter on cirrhosis
in this program. Alcoholic patients with cirrhosis may suddenly die of liver failure.
A superimposed hepatitis especially due to HCV is most often found in these cases.
separated from hemochromatosis which may occur in alcoholics.
5- HEPATOCELLULAR CARCINOMA
It arises in 5 to 15 % of alcoholic cirrhoses especially macronodular type. Macronodules
in alcoholic cirrhosis are the result of regenerative nodules which from hypaerplasia
may evolve into dysplasia, benign neoplasia (hepatocellular adenoma) and maignant
neoplasia (hepatocellular carcinoma). For the same reason, the incidence of
carcinoma is increased in cirrhotic patients with porta-cava shunt permitting the
nodules to receive more arterial blood favoring cellular growth.
6-ALCOHOLIC SIDEROSIS
Increased stainable iron is encountered sometimes in considerable amounts in most
alcoholics probably due to iron content of alcoholic beverages. Obviousely alcoholics
may be affected also by hemochromatosis.
7-ALCOHOLIC PHLEBOSCLEROSIS
In all cases of alcoholic hepatitis and alcoholic cirrhosis one of three types of
venous changes are seen:
1-Lymphocytic phlebitis
2-Perivenular fibrosis (of terminal central veins)
3-Veno-occlusive fibrosis (of large hepatic vein branches)
Portal hypertension correlates with the degree of phlebosclerosis.
8-ALCOHOL METABOLISM
Absorption. It is absorbed mostly in the duodenum and upper jejunum. Food
delays absorption. High concentration in the stomach may delay gastric emptying.
Distribution. It is related to the water content or various tissues. It is
poorly soluble in lipids, therefore a fat person has a higher blood concentration
of alcohol. Concentration in urine is higher than blood. Alcohol passes immediately
in highly vascularized organs. It passes immediately to the brain. It easily diffuses
to the fetus, the amniotic fluid acting as reservoir in utero.
Excretion: 95 % is eliminated by oxidation to water and carbon dioxide. About
3% is eliminated through the lungs. Very small amounts through the urine.
Catabolism. It oxidized mainly in the liver and much less in other organs
especially stomach , intestine, kidney , bone marrow. The oxidation proceeds in steps.
1-Alcohol to acetaldehyde in cytosol, microsomes and perixosomes.
2-Acetaldehyde to acetate in mitchondria.
3-Acetate to water, carbon dioxide, fatty acids in other tissues.
Transformation of alcohol to acetaldehyde occurs in three places.
1-Cytosol. Alcohol Dehydrogenase is the enzyme that catalyzes the oxidation
of ethanol and of all other alcohols to acetaldehyde in the cytosol. It catalyzes
also the oxidation of endogenous and exogenous steroids and omega oxidation of fatty
acids. This enzyme contains 4 atoms of zinc. By this reaction alcohol looses on atom
of hydrogen ad is transformed into acetaldehyde. The atom of hydrogen is accepted
by nicotinamide adenine dinucleotide (NAD) which becomes reduced to NADH. In order
to utilize again this cofactor for other important reaction, NADH must be reoxidised.
This reoxidation occurs in the mitochondria. But, if the mitochondria are damaged
by alcohol the reoxidation is prevented and an excess of reduced cofactor NADH is
produced and synthesis of other compounds such as proteins , lipids and carbohydrates
is impaired.
Microsomes. Microsomal Ethanol Oxidizing System (MEOS). This reaction
is catalyzed by a cytochrome P-450. The product is acetaldehyde. In chronic alcoholics
this metabolic pathway increases and apparently determines the increased tolerance
to alcohol of habitual drinkers.
Perixosomes. This reaction plays a lesser role. The reaction consists of oxidation
of ethanol with hydrogen peroxide with formation of acetaldehyde and water. It is
controlled by catalase.
CH-CH2OH+H2O2=CH-CHO+H2O
| ethanol | Acetaldehyde |