li-11-8
HEPATIC ALLOGRAFT REJECTION
by Dr. Grace Hartman
and Dr. E.Orfei
Classification
The
transplant
rejection in the liver is classified, as in other organs, in hyperacute, acute and
chronic.
In
liver transplants about
40% of patients prophylactically treated with cyclosporine and cortisone don't have any rejection; 40% will have one episode of rejection. Occasional patients
may have an accelerated rejection with massive liver necrosis, severe jaundice
and very elevated serum transaminases.
Hyperacute
rejection, antibody-mediated, is extremely rare in the case of liver transplant
with prophylactic immunosuppression, even in a mismatched case.
Acute rejection is rarely seen before the 4th post-transplant
day. It may
appear between the 4th and the 14th day after transplant. Some centers perform routine
liver biopsy on the 7th post-operative day because of the frequency of rejection
starting at that time.
Chronic
rejection may complicate an acute episode or may appear de novo after
several months an may persist for several months thereafter. It is usually
progressive.
Diagnosis
The
diagnosis is made by clinical symptoms, liver function tests and liver
biopsy.
Clinical
symptoms may be totally absent or may consist of fever , leukocytosis, jaundice and tenderness over the graft.
The leukocytosis will contain lymphoblasts.
Blood eosinophilia >500 eosinophils
/cubic mm in the blood is a good test and present in 98% of liver
transplants rejection.. Fine needle
aspiration with evaluation of presence of inflammatory cells could provide
valuable results in recognizing presence of rejection and in monitoring the
response to immunosuppression therapy.
Liver function
tests may show elevated serum bilirubin, aminotransferases, alkaline phosphatase and prothrombin
time.
Pathology
The
biopsy findings in liver transplant are the most complex of the hepatic pathology
because a transplanted liver besides cellular rejection may become affected by
other ailments such as: sepsis, biliary obstruction, arterial insufficiency, drug hepatitis caused by
immunosuppressive compounds and by hepatitis caused by viruses such as: HBV, HCV, CMV, EBV.
Pretransplant
biopsy of donor liver. There should be no portal expansion and no portal inflammation
and minimal portal fibrosis. Hepatocytes may show microvacuolization
especially in the pericentral area. Small foci of parenchymal necrosis my be
present, due to the trauma of harvesting and storage.
Post-transplant
baseline biopsy. Few neutrophils may be seen in the sinusoids, effect of
organ manipulation. The portal fields are normal. The hepatocytes look empty due to
microvacuolation.
Minimal
allograft rejection, "graft recognition". Presence of few lymphocytes in portal spaces, announcing an impending
rejection. The vacuolation of
hepatocytes
is disappearing.
Hyperacute
rejection: this primary humoral rejection, which can be observed within
minutes or hours after kidney transplant, is very rarely seen in liver
tranplants with prophylactic immunosuppression even in
mismatched cases. It is characterized by acute necrotizing vasculitis including
arterial thrombosis causing failure of the graft to become vascularizid. The
vascular lesion is induced by complexes of antibodies and histocompatibility
antigens released by injured cells during transplantation. This process ends in massive liver necrosis and
terminates in death. IgG, IgA, IgM antibodies and complement can be demonstrated
in the injured vessels by immunofluorescence. A florid atherosclerosis with
ballooned lipophages may develop in larger arteries, consequently the
transplanted organ
never becomes well vascularized and undergoes ischemic destruction.
Acute
hepatic rejection. It is graded in mild, moderate and severe.
Mild
acute rejection. There is mild portal inflammation and slight periportal inflammation with
mononuclear cells( helper T lymphocytes an suppressor/cytotoxic T lymphocytes),
some neutrophils and eosinophils.
There
is minimal
bile duct damage. Only some swelling or pyknosis of bile duct epithelium.
The hepatocye vacuolation has disappeared.
There may be bollooning of hepatocytes, focal necrosis and even bridging necrosis.
There is often centrolobular cholestasis.
Endothelialitis
is considered by some the most specific sign of rejection. It is
characterized by the adherence of small lymphocetes to the endothelium and
subendothelium of portal and central veins.
The
changes of rejection resemble those of Graft vs. Host Disease, but the latter
involves also. the skin and the intestine and it does not occur in transplants of
solid organs which are washed out of their lymphocytes.
Moderate
acute rejection. There is more bile duct damage. Swelling,
pyknois, cellular loss of ductal epithelium, lymphocytic infiltration of
epithelium. There is also more portal and periportal inflammation and more cholestasis.
Severe
acute rejection. Bile
duct degeneration is severe with disappearance of bile ducts and portal fibrosis
similar to the non-suppurative duct injury of graft-versus host disease and of
primary biliary cirrhosis Portal and periportal infllammation are
prominent. There may be endothelialitis of
portal an central veins. There is severe focal lobular necrosis of hepatocytes especially centrolobular with marked cholestasis.
Bile
ductules may be filled with bile plugs.
Vanishing
bile duct syndrome: About 10% of transplanted liver patients develop this
syndrome within 100 days after the procedure. The lesion is irreversible and
requires retransplantation.
It
starts abruptly with fever chills. jaundice, lethargy and ascites. Serum
bilirubin and alk. phosphatatse become very elevated
Histologically
there is marked ductopenia in " burnt out" portal areas devoid
of inflammatory cells. The few lymphocytes present are Leu 4+ and Leu 2a suppressor/cytotoxic
T .
Differential
Diagnosis
Other
conditions may affect the transplanted liver and may pose a difficulty in the
diagnosis of transplant rejection. These conditions are:
-Viral
hepatitis
-Massive
hepatic infarct due to thrombosis of hepatic artery.
-Thrombosis
of hepatic veins.
-Extrahepatic
biliary obstruction.
-Infectious
cholangitis.
-Parenchymal
cholestasis without inflammation , so-called functional graft failure.
-Reaction
to drugs especially to immunosuppressive agents.
-Recurrence
of primary liver disease.
-Insurgence
of malignancies especially of lymphoid organs, more frequent in
transplanted patients.
ILLUSTRATIONS
|
Fig .
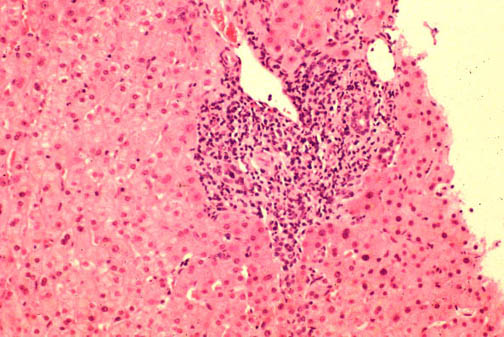
11-8-1. Acute rejection, moderate. .
11-8-1. Acute rejection, moderate.
Portal and
mild periportal inflammation with some neutrophils and eosinophils.
Moderate bile duct damage. Changes similar to Graft vs. Host Disease but
the later involves also the skin and the intestine.
|
|
Fig. 11-8- 2.
Severe acute rejection. 2.
Severe acute rejection.
Elimination
of intrlobular bile ducts. portal and periportal inflammation is lighter.
Bile ductules start to proliferate. Also portal fibrosis is evident
|
 Fig.
11-8-3. Vanishing portal bile ducts. Fig.
11-8-3. Vanishing portal bile ducts.
Marked
ductopenia. Few inflammatory cell, Leu4+ and Leu2a suppressor/cytotoxic
T.
|
|
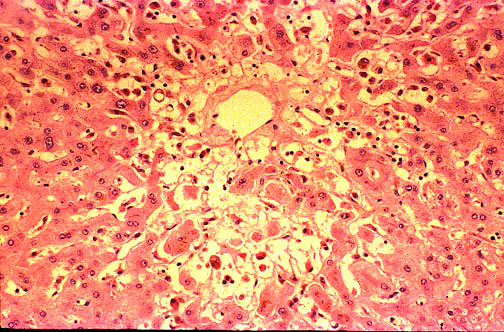
 Fig.11-8-4.Centrolobular
necrosis. Fig.11-8-4.Centrolobular
necrosis.
Spotty
necrosis may be seen in severe rejection. The necrosis is more
frequently present in centrolobular area |
|
 Fig.
11-8-5. Intralobular cholestasis. Fig.
11-8-5. Intralobular cholestasis.
Marked
centrolobular intacytoplasmic and canalicular cholestasis, clinically evident
with severe jaundice. |
|
 Fig.11-8-6.
Chronic vascular rejection. Fig.11-8-6.
Chronic vascular rejection.
Severe
arterial atheromatosis involving the entire length of the artery. It
starts with lymphocytic exudation of the intima which becomes
thickened and finally becomes invaded by cholesterol laden
macrophages. The transplanted organ suffers ischemic destruction.
|
TO
CONTENTS
Review of Pathology of the Liver:Table of Contents
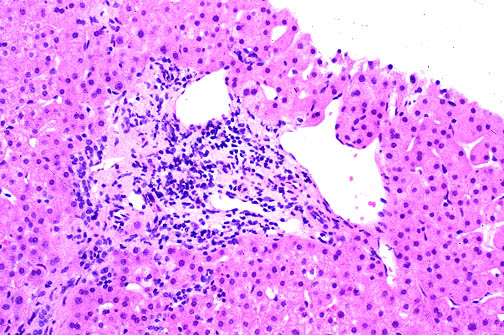 Fig.
11-8-3. Vanishing portal bile ducts.
Fig.
11-8-3. Vanishing portal bile ducts.