Definition
- ARDS is an acute pulmonary disorder characterized by diffuse capillary
leak resulting in wet lung and a constellation of features
secondary to it.
- This syndrome is associated with a multitude of clinical conditions
which primarily damage the lung or secondarily as part of a systemic disorder.
Pathogenesis
- ARDS is the end result of acute alveolar injury caused by a vareity of insults
and probably initiated by different mechanisms.
- The initial injury most frequently affects the endothelium, less
frequently the alveolar epithelium.
- There are many types of injuries which lead to the ultimate, common
pathway, i.e., damage to the alveolar capillary unit.
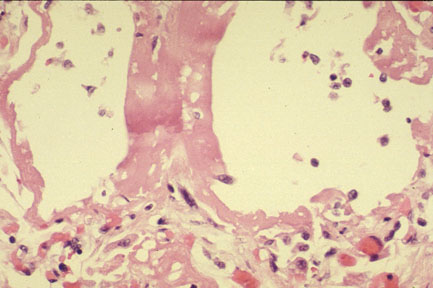
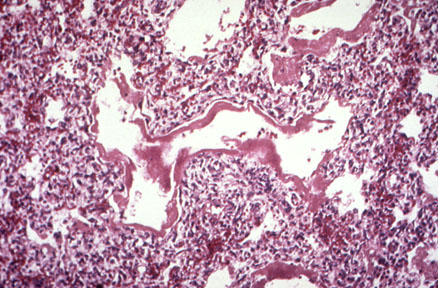
- Injury produces increased vascular permeability, edema,
fibrin-exudation (hyaline
membranes).
- Organization and scarring follows.
- Endotoxin, neutrophils, and macrophages may also play key roles in the
pathogenesis of ARDS
- Leukocytes (primarily neutrophils) plays a key role in endothelial damage.
- The capillary defect is produced by an interaction of inflammatory cells and
mediators, including leukocytes, cytokines, oxygen radicals, complement and arachidonate
metabolites, that damages the endothelium and allows fluid and proteins to leak.
Pathology
Pathophysiology
- There is diffuse loss of Surfactant resulting in alveolar
atelectasis.
- Lung becomes stiff and less compliant. Lung volumes decrease and
minute ventilation increases as a compensatory phenomenon.
- Tremendous intrapulmonary shunt develops as a consequence of
alveolar atelectasis, where there is no ventilation with respect to perfusion.
Clinical Features
- A major event always precedes. Common major events are Sepsis,
Shock, Trauma, Gastric aspiration, acute blood loss and acute Pancreatitis.
- Following a brief lag period of the major event, patient
develops hypoxia, tachypnea and rapidly progresses to acute hypoxemic respiratory
failure.
- Hypoxemia is refractory to therapy.
- CXR shows diffuse white out of lungs.
- Wedge pressure is normal indicating that it is non-cardiogenic
pulmonary edema.
Therapy
- Correction of the primary event that induced ARDS, if possible.
- Ventilator support to provide adequate oxygenation.
- PEEP is necessary to prevent alveolar atelectasis, decrease
shunt and improve oxygenation.
- Supportive care for nutrition and infections.
Prognosis
- Even with optimal therapy mortality is 60%.
- Patients who recover have almost normal pulmonary function. Some diffusion defect
can be residual.
{kind=link}
{kind=link}
{kind=link}