Definition
Bronchiectasis is a severe, chronic infection of the lung causing
pronounced permanent abnormal
dilatation of bronchi and bronchioles.
Pathology
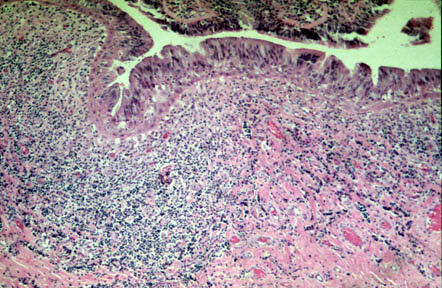
- Chronic, necrotizing infection of bronchi in a segment or multiple segments of
the lung.
- Infection damages and weakens walls of bronchi so that these
structures become markedly dilated
and filled with mucous and pus.
Pathogenesis
- The major factors which contribute to the development of bronchiectasis are loss
of muco-ciliary clearance system and infection.
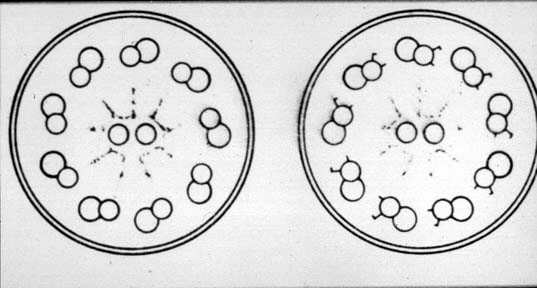
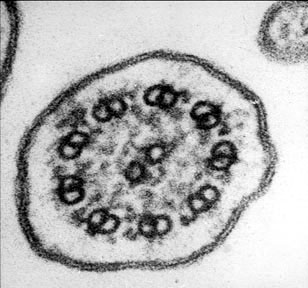
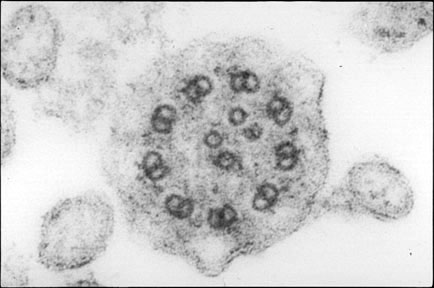
- The loss of muco-coliary escalator system can follow either obstruction (foreing
body) or due to defect in dyneim arm of cilia (Kertagener syndrome) or
due to abnormal mucus (Cystic fibrosis).
- Defect in the clearance mechanism is followed by accumulation of secretions,
bacterial overgrowth, infection and atelectasis.
- The chronic infection damages the integrity of the bronchial wall causing
dilatation.
- Temporary (6 Weeks) tubular bronchial dilatation occur in all pneumonias.
- Saccular bronchiectasis
follows destructive inflammation of the bronchial wall.
Pathophysiology
- The muco-ciliary escalator system is destroyed in bronchiectatic segemnts
perpetuating accumulation of secretions and infection.
- The bronchiectatic segments are also insensitive thus do not
provoke cough untill the pus spills over to normal bronchi.
- Airway obstruction follows diffuse bronchiectasis.
- If there is signifiacant recurrent pneumonias and peribronchial fibrosis
a restrive defect can be seen.
Localized vs. Diffuse Bronchiectasis
- Localized bronchiectasis is encountered under the following
clinical circumstances:
- Following necrotizing pneumonia
- Obstructive lesion
- Tuberculosis (dry bronchiectasis)
- Allergic bronchopulmonary aspergillosis
- Diffuse bronchiectasis is encountered in:
- Cystic fibrosis
- Immotile Cilia Syndrome (Kartagener's Trial) Cilia Cilia Cilia
- IgA deficiency
- Hypogammaglobulinemia
- Childhood infections
Clinical Features
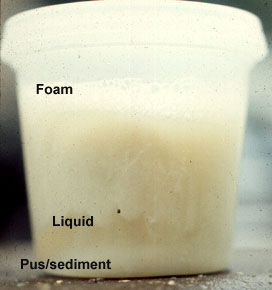
- Clinically characterized by postural cough and expectoration of large
quantities of foul smelling sputum with three characteristic layers. Fowl
smell is due to anaerobic infection. The three layers are purulant
sediment, clear middle liquid and top foamy layer. Bronchiectatic segments are insensitive
and do not provoke cough. When the patient bends down the gravity moves the pus to
proximal normal bronchi evoking a cough response, thus explaining the postural cough.
- Clubbing, coarse
persistent leathery rales are seen.
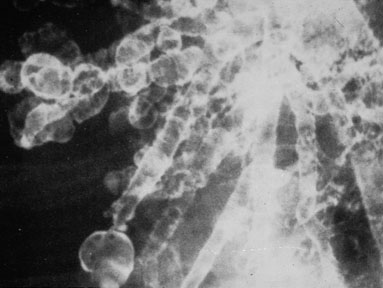
- Chest x-ray is often normal, but can show thickened bronchial
walls, multiple cystic spaces with airfluid levels.
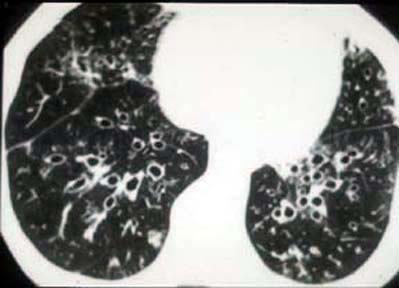
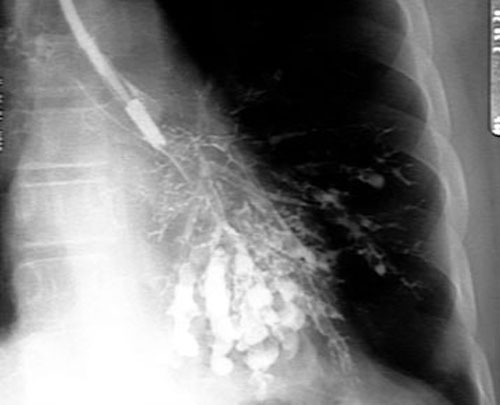
- Characteristic dilated bronchi can be demonstrated with high
resolution CT. Bronchogram
is no longer necessary.
- A combined obstructive and restrictive defect can be seen in PFT's.
- Superimposed infection may be present, e.g., aspergillosis
Therapy
- Localized bronchiectasis can be cured with resection, if
indicated.
- Cyclical antibiotics and postural drainage are
the mainstay of therapeutic measures for diffuse bronchiectasis.
- Lung transplant is an option for far advanced cases.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}