Anatomy
Serous Membrane
Visceral and parietal division, approximately equal surface area. Each is 1 layer of
mesothelial cells, basement membrane, connective tissue, microvessels and lymphatics
Mesothelial Cells
Single layer, pleomorphic. Surface microvilli, more dense on visceral side of pleura
Stomata
Opening between cells, 2-12 um, only on the parietal surface. The usual exits into
lymphatic lacunae for liquid, protein, and cells
Blood Supply
Some controversy. Human visceral pleura supplied by systemic bronchial vessels, drain
through fairly large capillaries to pulmonary veins. Parietal blood from adjacent chest
wall, drainage to bronchial veins; diaphragmatic pleura supply from nearby arteries,
drainage to inferior vena cava and brachiocephalic trunk
Lymphatics
More dense lower and toward the mediastinum. Drainage toward hilum either via lung or
pleura itself. Stomata lead to lacunae which form valves. Drain to mediastinum via
intercostal route depending on origin. Visceral pleural drainage to middle mediastinal
nodes or posterior (lower lobes)
Physiologic Principles
Misconceptions or Recent Advances
- Visceral pleural blood from pulmonary circuit - really from bronchial supply
- Absorption of protein-free fluid via visceral pleura - really absorbed through
stomata on parietal surface.
- High rate of normal fluid and protein turnover - actually very low rate
True Concepts
- Fluid formed at parietal surface - Pressure gradient from parietal pleural
intestinum to pleural space due to subatmospheric pleural space pressure. Little from
visceral surface.
- Pleural protein filtered to 0.3-9.4 g/dl, then water reabsorbed leaving 1-1.5
g/dl
- Lower filtration rate found with radiolabeled albumin studies in sheep by Staub,
et al. Old data, likely due to model (dog) and inflammation from pleural catheters.
Lymphatics with large reserve - if fluid accumulates, there is both increased fluid
formation and decreased clearance
- Six mechanisms of pleural fluid accumulation
- Increased hydrostatic pressure, especially systemic venous pressure combined with
capillary wedge pressure in CHF
- Decreased oncotic pressure - by itself not a huge problem because of lymphatic
reserves
- Decreased (more negative) pleural pressure - collapsed or trapped lung
- Increased permeability of microvasculature, inflammatory fluid formation
- Impaired lymphatic drainage - blockage of channels with tumor, fibrosis, etc.
- Fluid from peritoneal space - ascites moves via diaphragmatic lymphatics or
diaphragmatic defects (less than 1 cm)
- Gas absorption - dependent on N2 gradient. In pneumothorax, 02 therapy increases
gradient of N2 from pleural space to venous blood
- The lower limit of pleura is 10th interspace posteriorly and 6th anteriorly.
Hence gravity facilitates accumulation of fluid in the gutter
posteriorly first.
- With most etiologies (except negative pressure induced pleural effusion) once the
fluid accumulates in pleural space the negative pressure decreases and
eventually becomes positive.
- Loss of negative pressure in pleural space results in higher resting
position of hemithorax.
- The lung relaxes and becomes smaller since there is no negative
pressure to hold it close to chest wall.
- Once the pressure becomes positive the mediastinum and diaphragm get pushed.
- The diaphragm eventually can become concave upwards.
- Fluid is subpulmonic to start with the lung relaxes and floats attached to hilum.
As the lung retracts towards hilum, fluid tracks up between visceral and parietal pleura.
Fluid has a broad base and thin apex along the chest circumference. The meniscus
appearance of the fluid is a visual illusion, thickness of fluid level is higher along
sides compared to the middle.
- Fluid moves freely and shifts with position.
- As the pleural pressure increases with more fluid formation i.e. massive pleural
effusion the lung becomes completely atelectatic. Airways are patent. Fluid is a
good conductor of sound.
Radiology
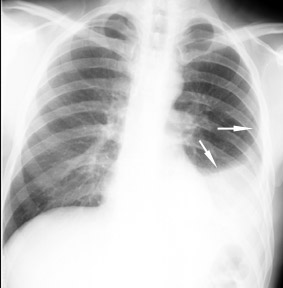
Fluid
accumulates in pleural space.
Irrespective of the nature of fluid, radiologically they will look similar. You
are looking at pleural effusion on left.
Radiological criteria are:
- Density
- In dependent portion
- Costophrenic angle in PA view
- Anterior and posterior portions of gutter in lateral view
- Along sides in lateral decubitus position
- Along posteriorly in supine position, giving diffuse haziness on the side of
effusion
- Silouhette of upper limit of density
Compare the Costophrenic angle before
and after
clearance of effusion.
Note also lack of identifiable left diaphragm before and visible diaphragm after
clearance of fluid (Silouhette sign principle).
Pleural Effusion
Physical Findings
- Mediastinum
is in midline to start with and gradually gets shifted to opposite site as the pleural
pressure becomes positive.
- Chest Expansion decreases on the side of effusion due to
decreased ventilation.
- Resonance is dull and flat to percussion. Dullness is most in
posterior base in erect position. Flatness is recognized by tapping the chest with flat of
your hand. Traubes space will be obliterated on left sided effusions.
- Breath Sounds are decreased since the ventilation to that
hemithorax is decreased. Fluid is a good conductor of sound. If there is underlying
consolidation a good bronchial breathing will be heard over the effusion. In massive
effusions with completely atelectic lung and patent airways one can also hear bronchial
breathing over the effusion.
- Voice Transmission decreases and follows breath sound
characteristics. Egophony
is noted along the upper margin of the fluid. This is probably due to a thin film of
fluid separating pleural space.
- Adventitious Sounds: None
- Hemithorax size is larger due to loss of negative pressure in
pleural space.
- Effort of Ventilation: Respiratory rate increases and use of
accessory muscles can be recognized.
- Effect on Function: Can lead to central cyanosis.
Pleural Fluid Analysis (Diagnostic Tests)
Thoracentesis
- Indications: effusion without a secure clinical diagnosis (e.g., CHF) or small
quantity
- Contraindications: none absolute, relative risk > benefit, bleeding diathesis,
small effusion, mechanical ventilation, anticoagulation
- Complications:
- Subjective: anxiety, site pain
- Objective: pneumothorax (12% at a University H), 1/3-1/2 of those require check
tubes; fluid contaminated with blood, "dry tap"; empyema; puncture of other
organs (e.g., liver); hypoxemia and unilateral pulmonary edema only with therapeutic taps
- usually large and occur with carcinoma or trapped lung
- Benefit: relief of dyspnea with therapeutic tape - via reduction of chest wall
size even though hypoxemia occurs
- Diagnostic yield:
- Almost 75% of thoracentesis yield a specific or presumptive diagnosis; 15-20%
more are useful in management (e.g., rule out empyema)
- Specific diagnoses: malignancy (cells), empyema (pus), tuberculosis pleurisy
(AFB), fungal infection (KOH), lupus pleuritis (LE cells), chylothorax, urinothorax fluid
creatinine/serum creatinine greater than 1), esophageal rupture (high fluid amylase, Ph
about 6.0)
- Tests that should be run (35-50 ml fluid): LDH, protein, WBC count and
differential, glucose, Ph; concomitant serum protein, LDH, glucose; arterial pH if fluid
pH <7.30 and acidemia is suspected. Supplement with other reasonably requested analyses cytology, cultures, smears, immunology, amylase, lipids, CEA, etc.
- Results:
- Exudate vs. transudate:
(1) Fluid/serum protein ratio > 0.5
(2) Fluid/serum LDH ration > 0.6
(3) Fluid LDH > 2/3 upper normal serum LDH; exudates have 1 or more; transudates none
these characteristics
- If LDH only is abnormal - consider malignancy or parapneumonic effusion
- Protein may confuse: e.g., CHF <3 g/dl, but might be 3-4 g/dl if patient uses diuretics, or is chronic or recurrent
- WBC: rarely diagnostic alone; > 50,000 in
parapneumonic effusion, usually empyema; > 10,000 very inflammatory
(1) Early, acute, PMN predominant
(2) Later mononuclear - high counts suggest TB, carcinoma, lymphoma, sarcoidosis
(3) Eosinophilia - 10% suggest benign, self- limited; commonly with air or blood in
pleural space; consider: hemothorax, pulmonary infarction, pneumothorax, previous
thoracentesis, parasitic diseases, fungi, drugs, asbestos; rare with TB or malignancy. In
1/3 "idiopathic"
(4) Basophilia - 10%, rare; suggest leukemia
- Mesothelial cells - paucity of cells occurs with chronic diffuse pleural lesions,
e.g., TB, malignancy, empyema rheumatoid effusion, pleurodesis. If > 5%, essentially
rules out TB
- Bloody (> 100,000 cells/mm3): malignancy, trauma, pulmonary embolism,
post-cardiac injury, asbestos pleurisy
- Cytology: yields nearly 90% with malignancy as cause
Percutaneous Pleural Biopsy
- Indication: undiagnosed exudate, especially lymphocytic (yield: TB - 75%, over
90% with AFB culture of tissue; malignant 60%)
- Contraindications: obliterated pleural space, anticoagulation, uncooperative
patient, bleeding diathesis
- Complications: similar to thoracentesis
Thoracoscopy
- Indications: controversial because it usually requires hospitalization, and only
increased yield a small amount. Pleurodesis can be done at the same time
- Contraindications: like closed biopsy
- Complications: tumor seeding common
Open Biopsy
- With thoracotomy and autopsy, the "gold" standard - but risk and cost
are relatively high
Specific Diagnoses
Transudates
- CHF, cirrhosis, peritoneal dialysis, urinothorax, nephrotic syndrome, atelectasis
Selected Exudates (There are many other causes besides these )
- Parapneumonic - uncomplicated: LDH <700, glucose="serum," pH> 7.30
- Parapneumonic - complicated: LDH > 1000, glucose <40, pH < 7.10
- TB - lymphocytic exudate;
pleural biopsy is diagnostic
- Carcinoma - bloody, lymphocytic exudate, cytology or biopsy positive; if LDH only
is abnormal - think cancer; pH <7.30 associated with poor prognosis and poor response to sclerotherapy
- Esophageal perforation - pH 6.00, high amylase (salivary)
- Rheumatoid pleurisy - turbid, yellow-green, debris- laden fluid; LDH > 1000,
glucose <30, pH 7.00, RF> 1:320
- Lupus - LE cells in effusion (increase if fluid sits up to 24 hours):
occasionally low glucose and pH
- Post-cardiac injury syndrome - pleuritic pain, rub, fever 3 weeks after injury;
left infiltrates, serosanguineous - no diagnostic labs
- Pulmonary embolism - nothing characteristic; fluid maximal by 72 hours
- Pancreatitis - usually left sided, pleural fluid amylase: serum amylase > 1.0;
amylase may be > 100,000 with pseudocyst
- Asbestos pleural effusion - asymptomatic; bloody exudate, unilateral
- Trapped lung - unilateral; serous, "borderline" exudate, very low
pleural liquid pressure, rapid reaccumulation
- Chylothorax - lymphocytic, milky; chylomicrons in fluid, TG > 110 mg/dl
- Lymphangiomyomatosis - chylothorax in a young women, interstitial disease, normal
lung volumes, repeated pneumothoraces
- Yellow nail syndrome - 40 years old with yellow nails, lymphedema, respiratory
tract involvement, triad not simultaneous; pleurodesis effective
References
- Light RW: Pleural Disease, 2nd edition. Philadelphia, Lea and Febiger, 1990.
- Light, RW et al: Parapneumonic effusions. Am J Med 69:985- 986, 1980.
- Sahn SA: State of the art: The pleura. Am Rev Respir Dis 138:184-234, 1988.
- Sahn, SA, Good, JT Jr: Pleural fluid pH in malignant effusions. Ann Intern Med
108:345-349, 1988.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}