Pathologic Principles
It is extremely important to have a good understanding of Pathological processes
that occur if one desires to pick them up by physical exam. Each organ or tissue responds
in only certain ways for offending agents. Same type of pathological responses are often
seen with different etiologies.
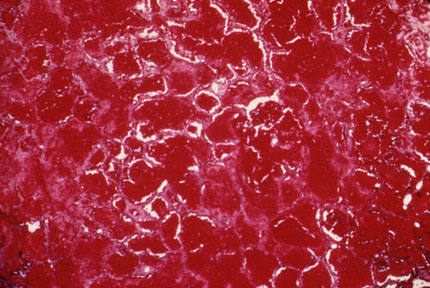
The Lungs - Diffuse
- Alveolar
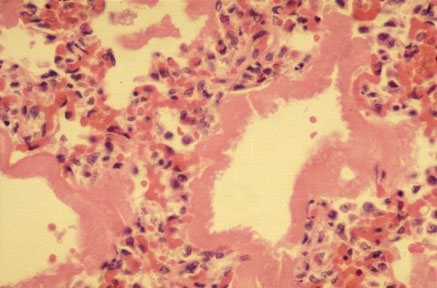
In this pathological process the alveoli, diffusely in both lungs are filled with either
water (pulmonary edema), blood or inflammatory
exudate. The interstitium is normal. Hyaline
membrane can form along alveolar wall. The elastic recoil increases and the size of
the lung decreases. There is decreased compliance and lung expansion decreases.
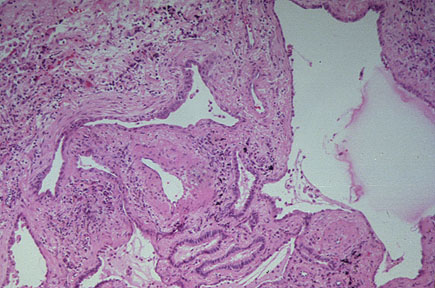
- Interstitial
The interstitium consists of lymphatics, capillary bed . Diseases of any of these
structures can cause thickening. Water (pulmonary
edema), lymphatic engorgement, blood, inflammatory exudate and fibroblasts can be the
cause for the thickening. Lung becomes heavy. The elastic recoil increases resulting in
smaller lung. Lungs become stiff and expansion decreases.
Localized
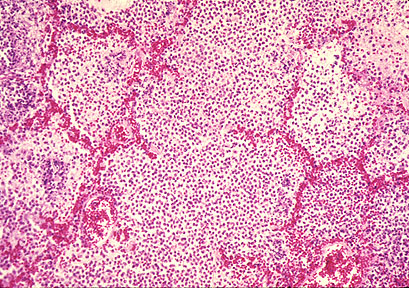
- Consolidation
The process involves a segment or a
lobe. The
alveoli are filled with inflammatory exudate.
Pneumonia goes through stage of red hepatization when the alveoli are predominantly filled
with red cells. Polymorphs and organisms can be seen in the alveoli. The visceral pleura
becomes irregular and inflamed. The size of the lobe initially slightly swells and
gradually decreases slightly. There is no significant loss of lung volume in
consolidation. the airways are patent except for mucus or pus in the stage of resolution.
Depending on the nature of offending organism or agent there may be necrosis of lung
tissue.
- Atelectasis
Atelectasis means alveoli devoid of air. There are four types of atelectasis.
- Absorptive: When there is airway occlusion, there is no more
ventilation to lung beyond obstruction. Gradually the air gets absorbed by the pulmonary
circulation. The lung collapses. This results in loss of lung volume on that side.
- Relaxation: The lung is held in opposition to chest wall because of the
negative pressure in the pleural space. Once this negative pressure is lost as in
pneumothorax or effusion the lung relaxes to its resting state.
- Adhesive: Alveoli are kept open by surfactant. If for any reason the
surfactant is depleted the alveoli collapse. In ARDS there is diffuse adhesive
atelectasis. In pulmonary embolism you get plate like atelectasis due to loss of CO2 and
surfactant.
- Contractile: In fibrosis the alveoli are squeezed out of their air.
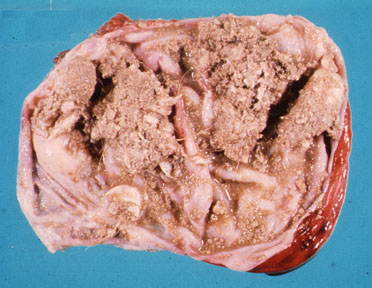
- Mass
- This is a space occupying lesion. There is no lung architecture. The cut surface is homogenous. Margins are sharp. The
lesion may not respect fissures. The lesion can infiltrate invade or compress surrounding
structures.
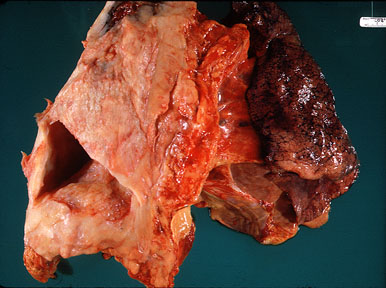
- Cavitation
- Cavity is a hole in the lung. It has
wall which can be made up of necrotic tumor or inflammatory mass. The lumen may be
irregular. it can be either empty or filled with pus, blood, necrotic debris, or fungus
ball. The cavity can be completely filled. There may or may not be a communication to
bronchus.
- Fibrosis
- The lung is focally fibrotic. There is loss of lung volume.
- Congestion
- The bases of lungs are congested and heavy.
- Distension
- In patients with COPD, Asthma and Emphysema the alveoli are dilated or distended. The lungs are
larger either due to loss of elastic recoil as in emphysema or due to air trapping as in
Asthma. There may be blebs in Emphysema. Most of these blebs are superficial and along the
upper lobes.
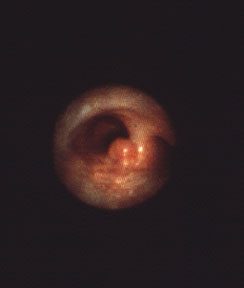
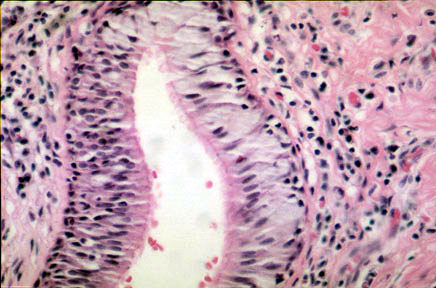
Airways
Pleura
Mediastinum
Chest Wall
- Deformity
- Mass
- Inflammation
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}