Definition
Bronchogenic carcinoma is a malignant neoplasm
of the lung arising from the epithelium of the bronchus or bronchiole.
Pathology
Bronchogenic carcinomas begin as a small focus of atypical epithelial cells within the
bronchial mucosa. As the lesion progresses, the atypia becomes frankly malignant and the
neoplasm grows in size. The neoplasm may grow into the bronchial lumen, along the mucosa
or into the bronchial wall and adjacent lung parenchyma.
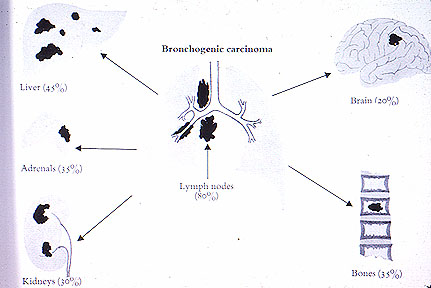
Eventually the neoplasm spreads to regional lymph nodes
and distant organs such as the liver, brain and bone.
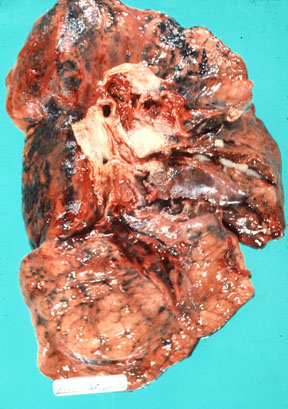
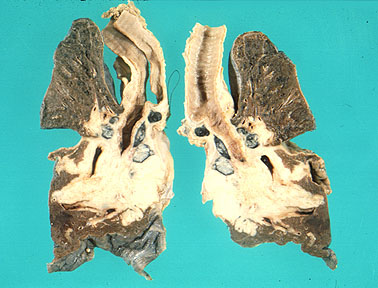
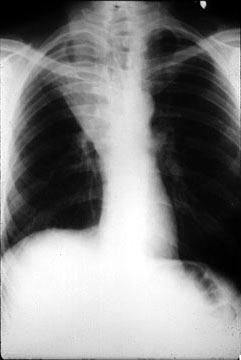
Most bronchogenic carcinomas form a mass in or near the
hilus. Some neoplasms, especially the adenocarcinomas, form a mass in the periphery of
the lung. Refer to Figure 15-42 in your textbook. The following classification scheme
represents the major histologic types of bronchogenic carcinoma. Refer to Table 15-10 in
your textbook.
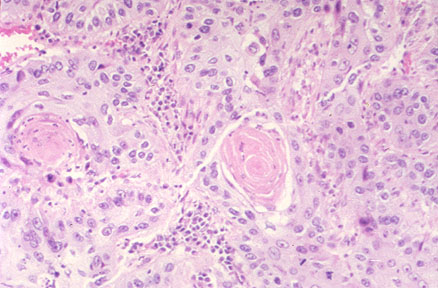
- Squamous Cell Carcinoma:
The neoplasm is composed of malignant squamous cells which may vary in degree of
differentiation from tumor to tumor. A well differentiated squamous cell carcinoma may
form keratin and intercellular bridges. Refer to Figure 15- 44 in your textbook. CLINICAL
NOTE: This neoplasm is most common in men and is closely related to smoking.
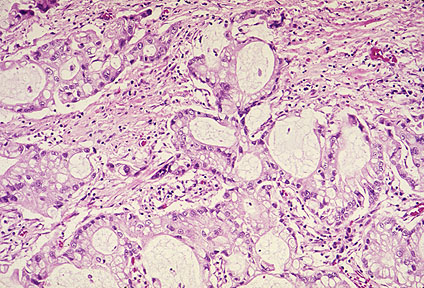
- Adenocarcinoma: The
neoplasm is composed of malignant glandular epithelium which may vary in degree of
differentiation from tumor to tumor. Well differentiated neoplasms may form distinct
glands, other neoplasms may vary from forming papillary structures to solid neoplasms
without any gland formation. Adenocarcinomas tend to be smaller than other bronchogenic
carcinomas and located in the periphery of the lung. A distinctive type of adenocarcinoma
is bronchioloalveolar carcinoma. CLINICAL NOTE: This
neoplasm is the most common type in women and nonsmokers.
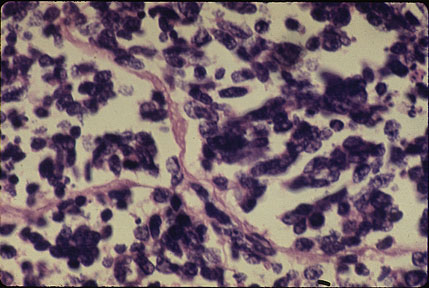
- Small cell carcinoma: The
neoplasm is composed of small cells containing dark
blue, round nuclei and sparse cytoplasm. These cells resemble (but are not) lymphocytes
and are arranged in clusters. Refer to Figure 15-43 in your textbook. Electron microscopy
reveals that these cells contain neurosecretory granules, indicating their origin from
neuroendocrine cells. Refer to Figure 15-44 in your textbook. CLINICAL NOTE: This neoplasm
is strongly related to smoking. It is a very aggressive neoplasm, generally having
metastasized at the time of diagnosis.
- Large cell carcinoma: The neoplasm is composed of large,
undifferentiated malignant cells.
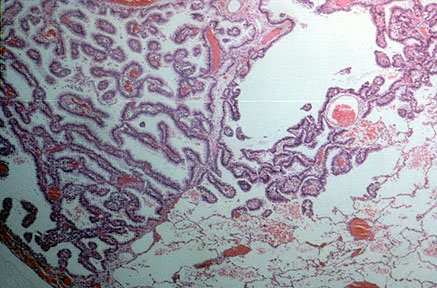
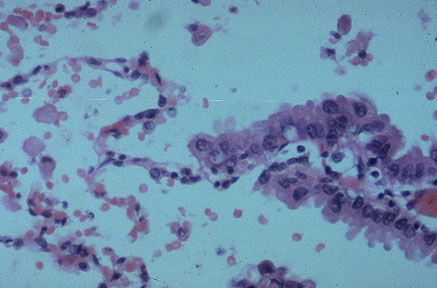
- Bronchioloalveolar carcinoma:
The neoplasm is a distinctive form of adenocarcinoma. The neoplasm arises from the
epithelium of the terminal bronchiole or the alveolus. The neoplastic cells are columnar, lining alveoli or form palliary growths which project
into the alveolus. Refer to Figure 15-45 in your textbook. The neoplasm, almost always
arising in the periphery, is solitary or forms multiple coalescing nodules.
Pathophysiology
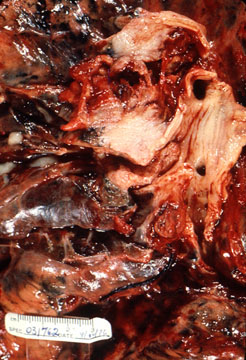
- Bronchogenic carcinoma tends to form an intraluminal mass which may partially or completely obstruct the bronchus. The neoplasm also may
compress or invade local structures such as aorta, esophagus, superior vena cava or
cervical sympathetic chain. What are the clinicopathologic consequences of obstruction or
invasion?
- Bronchogenic carcinoma may present with a variety clinical manifestations but the
major findings are cough, weight loss, chest pain and dyspnea. These neoplasms also have
the capacity to secrete hormones or hormone-like substances which have a variety of
clinical effects.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}