Learning Objectives: You should be able to:
- Explain the deceleration/acceleration of air in terms of
three air flow profiles that occur during each inspiratory/expiratory half
cycle.
- List the four primary factors that affect the prevailing
airway resistance centrally and peripherally.
- Diagram how forced expirations cause flow limitations at
lung volumes below FRC in exact accordance with a Starling resistor model.
- Name the two major components contributing to the work of
breathing and show how each is altered in different disease states.
Rhoades & Tanner Text Readings: Chapter 19, Pages 352-362
Airflow Profiles
Dynamic Compression
Air-Flow Resistance
Work of Breathing
MainMenu
Air Flow Profiles in the Airways
- Cross-Sectional Area of
the Airways
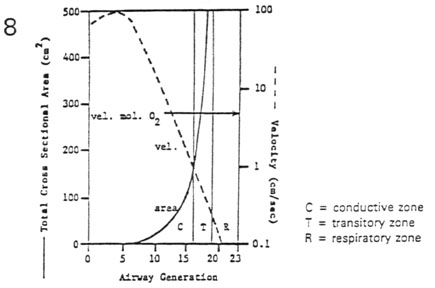
- total cross-sectional area increases exponentially with
generation (solid line)
- forward air flow velocity decreases exponentially with
generation (dashed line)
- Three Types of Air-Flow Profiles
- continuity equation
- flow (mL/sec) = vel (cm/sec) * cross-sect area (cm2)
* (mL/cm3)
- Reynold's Number (NR) = density * mean
velocity * diameter / viscosity
- turbulent flow for NR > 3000 (gen. 0-6)
- laminar flow for NR < 2000 (gen. 7-17)
- diffusive flow with cardiogenic mixing for NR
= 0 (gen. 18-23)
Airflow Profiles
Dynamic Compression
Air-Flow Resistance
Work of Breathing
MainMenu
Dynamic Compression of the Airways
- Flow-Volume Loops
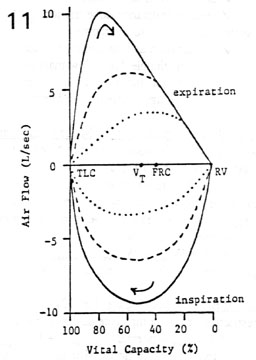
- air flow (L/sec) is plotted against lung volume (%
Vital Capacity)
- inspiratory and expiratory air flows form a closed loop
(clockwise rotation)
- for any lung volume, max inspiratory air flow is effort
dependent
- for high lung volumes, max expiratory air flow is
effort dependent
- for low lung volumes, max expiratory air flow is effort
independent
- Dynamic Compression of the Airways
- the expiratory portion of the maximal flow-volume loop
has a scooped- out appearance
- during active, forced expiration Ppleural
can actually exceed Pairway
- this transmural pressure gradient favors airway
compression (Starling resistor effect)
- greater effort (
 Ppleural) results in greater compression (
Ppleural) results in greater compression ( radius) with no change in air flow
radius) with no change in air flow
- compression starts at the equal-pressure point (EPP) in
the cartilage-free airways within the lung
- in disease the weakened airways can actually collapse
causing air-trapping behind the blockade
- lip pursing moves the EPP to the mouth, a psychological
relief to the patient
Airflow Profiles
Dynamic Compression
Air-Flow Resistance
Work of Breathing
MainMenu
Four Factors Affecting Air-Flow Resistance
- Airway Caliber
- laminar flow (
 )
=
)
=  pressure (P) / resistance (R)
pressure (P) / resistance (R)
- slope of line = 1/R = conductance
- resistance (R) to laminar flow
 1/radius4
1/radius4
-
airway caliber (secretions, bronchoconstriction): <
R and <
P
- Air-Flow Profile
- laminar flow (<)
increases linearly with <
driving pressure
- non-laminar flow (<)
increases curvilinearly with <
driving pressure
- Rnon-laminar flow is effectively greater
than Rlaminar flow due to turbulence
- for any given <
P, <non-laminar
< <laminar
- or any given <,
<Pnon-laminar
> <
Plaminar
- Airway Generation

- in general, regional airway resistance decreases as a
function of airway generation
- in specific, the highest regional resistance is at
generation 4
- medium sized bronchi of short length and frequent
branchings highly non-laminar air flow with extreme turbulence
- Lung Volume
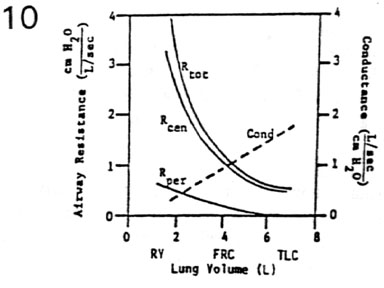
- total airway resistance = summation of serial regional
resistances
- Rtotal decreases hyperbolically with
increases in lung volume
- conductancetotal increases linearly with
increases in lung volume (dashed line)
- increases in lung volume cause increases in radius
due to tethering of the airways
- Rtotal can be partitioned into two
components
- Rperipheral (gen. 7 - gen. 23): low
resistance (laminar & diffusive zones)
- Rcentral (nose - gen. 6): high
resistance (turbulent flow zone)
- Rcentral >>> Rperipheral
(50% of resistance in nasal passages alone)
Airflow Profiles
Dynamic Compression
Air-Flow Resistance
Work of Breathing
MainMenu
Work of Breathing
- Components of Work
- elastic work - work to overcome:
- lung elastic recoil
- thoracic cage displacement
- abdominal organ displacement
- frictional work - work to overcome:
- air-flow resistance (major)
- viscous resistance (lobe friction, minor)
- inertial work - work to overcome:
- acceleration and deceleration of air (negligible
due to low mass of air)
- acceleration and deceleration of chest wall and
lungs (negligible due to overdamping)
- Graphical
Representation of the Major Components of Work
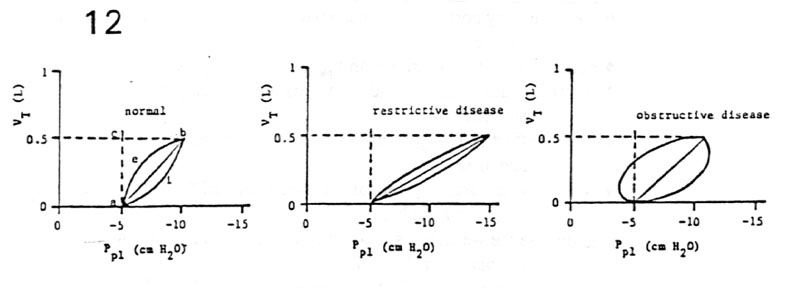
- work = force * distance
 pressure * volume / 2
pressure * volume / 2
- elastic work
area a-b-c-a
- inspiratory flow-resistive work
area a-i-b-a
- expiratory flow-resistive work
area a-b-e-a
- negative work
area a-e-b-c-a (tone on inspiratory muscles during expiratory air flow)
- total work
Welastic + Winspiratory flow-resistive + Wnegative
- passive recoil of lungs overcomes the work of
expiratory flow-resistance
- Work of Breathing in Disease (Fig. 12)
- restrictive or low compliance diseases (e.g. fibrosis)
Welastic + normal Wflow-resistive +
Wnegative =
Wtotal
- obstructive or high air flow resistance diseases (e.g.
asthma)
normal Welastic +
Wflow-resistive +
Wnegative =
Wtotal
Airflow Profiles
Dynamic Compression
Air-Flow Resistance
Work of Breathing
MainMenu


