
|
|
Thorax - Lymphadenopathy |
A large majority of patients have lymphadenopathy visible on radiographs and even more on computed tomography. When evaluating the hila for lymph node enlargement, special attention should be given to the lateral chest radiograph. Questionable abnormalities can be further evaluated with computed tomography if necessary.
In most patients lymphadenopathy resolves spontaneously, but the lymph nodes may stay enlarged for years. Some patients with Stage I sarcoid have had regression of lymph node enlargement, but then developed lymphadenopathy a second time.
Hilar lymphadenopathy has not been found to develop or increase after a patient has presented with Stage III sarcoidosis. If a patient with only parenchymal lung disease on a chest radiograph developes or has an increase in lymphadenopathy, the patient either has an incorrect diagnosis or a second disease .
Lymphadenopathy in the thorax due to sarcoidosis can be indistinguishable from other diseases, especially lymphoma and chronic infections. Unilateral hilar lymphadenopathy and mediastinal lymphadenopathy without hilar lymphadenopathy are infrequent in sarcoidosis and usually indicate another disease. Even the classic pattern of bilateral symmetric hilar and mediastinal lymphadenopathy due to sarcoidosis can be duplicated by other diseases including lymphoma. No pattern is pathognomic.
| MOST COMMON PATTERN | LYMPHADENOPATHY ON CT |
|---|---|

|
|
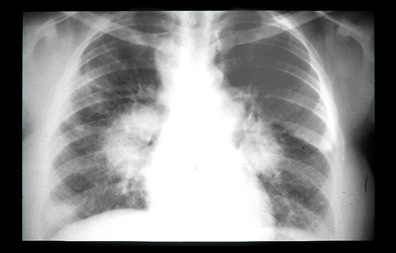
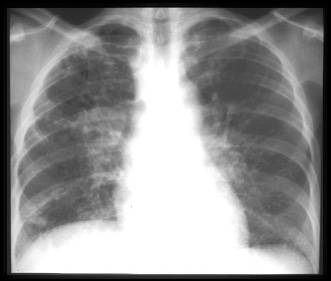
Bilateral symmetric hilar and right paratracheal mediastinal adenopathy, as in this patient, is the most common pattern of lymphadenopathy in sarcoidosis. |
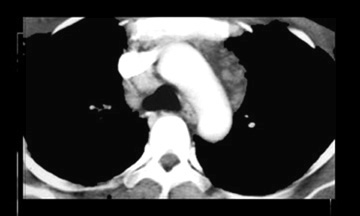
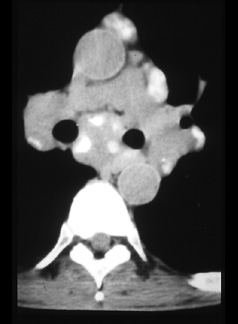
Computed tomography shows para-aortic and retrocaval lymphadenopathy. CT can demostrate enlarged lymph nodes which are not visible on radiographs. |
| PARACARDIAC LYMPH NODE | POSTERIOR MEDIASTINAL LYMPH NODE |
|---|---|
|
|
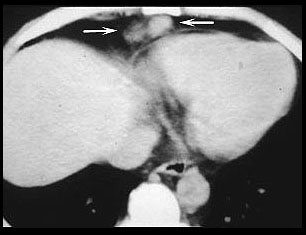
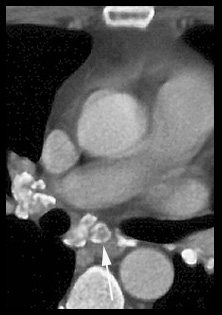
There is an enlarged right paracardiac lymph node (arrows). CT shows more lymph nodes than radiographs and more accurately locates the nodes. This is important in deciding which procedure should be used; mediastinoscopy, bronchoscopy, Chamberlin procedure, or percutaneous biopsy, if it is necessary to biopsy a node. |
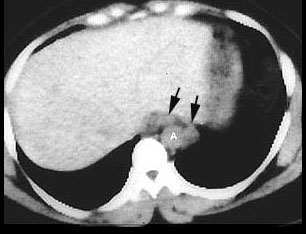
An abnormal radiograph of an asymptomatic nurse led to a CT study . CT showed these enlarged posterior mediastinal lymph nodes (arrows) next to the aorta (A). Bilateral hilar adenopathy was also shown. The posterior mediastinum is the least common site of adenopathy in sarcoidosis, but transbronchial biopsy showed nonceaseating granulomas. The nurse remains asymptomatic ten years later. |
| ADENOPATHY AT TIME OF DIAGNOSIS | ADENOPATHY DECREASED 2 YEARS LATER |
|---|---|
|
|
At the time of diagnosis there are marked enlarged hilar and mediastinal lymph nodes. |
Two years later the lymph nodes are smaller and there is parenchymal lung disease.
|
| CALCIFIED LYMPH NODES | EGGSHELL CALCIFICATION |
|---|---|
|
|
Calcified lymph nodes, as in this patient, are a late manifestation in 5% of patients. |
Lymph nodes with rim (eggshell) calcification (arrow) are rare in sarcoidosis but common in silicosis. |



| Terrence C. Demos, M.D. |
Last Updated: March 14, 1996 Created: March 1, 1996 |